

What is rectum and rectal Cancer?

The rectum is the last part of the gastrointestinal tract. Rectal cancer and colon cancer are generally clubbed together and discussed as colorectal cancer. However, there are many important differences. Mainly because rectum sits in a narrow cavity called pelvis barely separated from adjacent organs and bone. Moreover, many times the tumour is very close to the anal sphincter (the muscle ring responsible for holding the stools in the rectum). Because of these, the treatment of rectal cancer differs from colon cancer.
What are the signs and symptoms of rectal cancer?
These cancers like most other gastrointestinal cancers are asymptomatic in initial stages.
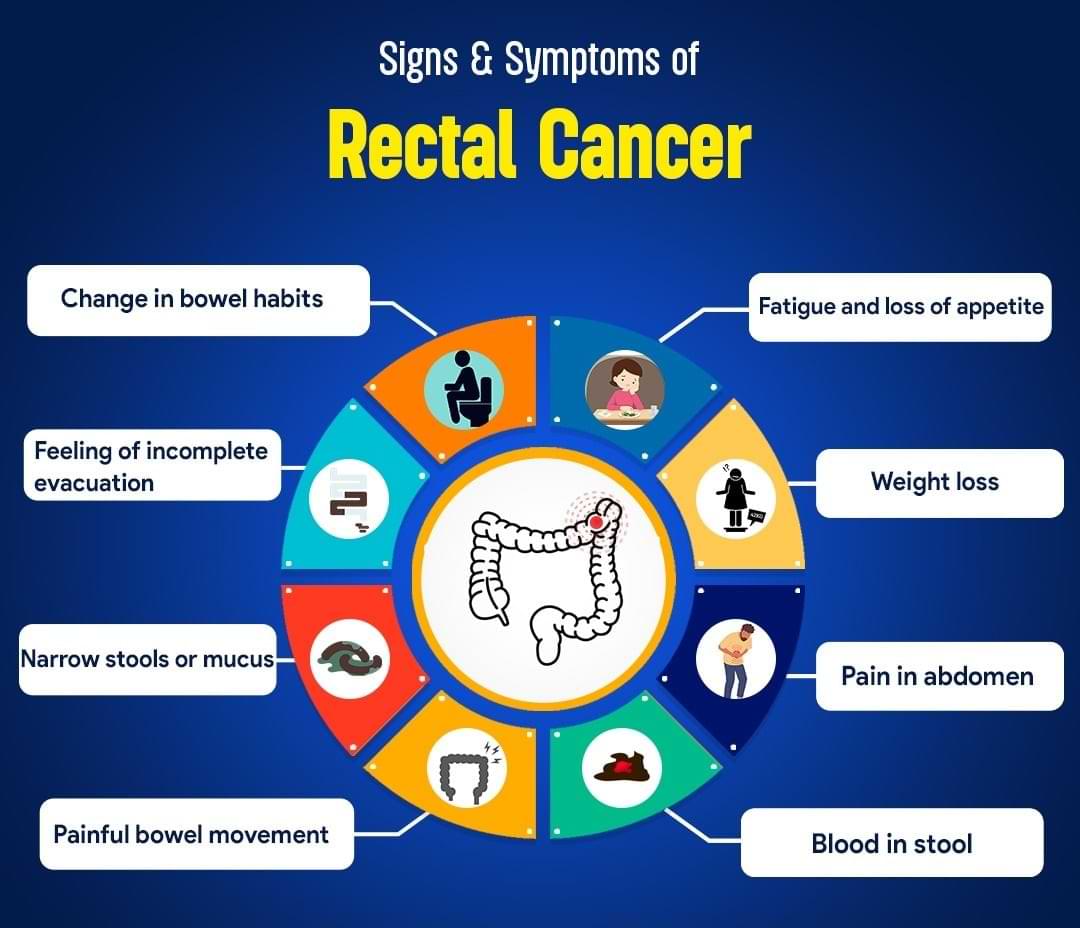
The symptoms of rectal cancer include:
- Change in bowel habits; persistent diarrhoea or constipation
- Feeling of incomplete evacuation
- Narrow stools or mucus in stool
- Painful bowel movements
- Unexplained fatigue and loss of appetite
- Unintentional weight loss
- Fall in haemoglobin (anemia)
- Pain or discomfort in abdomen
- Patches of dark blood in stool
What are risk factors of rectal cancer?

Some gene mutations run in families and increase the risk of colorectal cancer. The most common inherited colon cancer syndromes are:
Risk factors for rectal cancer are:
- Hereditary nonpolyposis colorectal cancer (HNPCC): HNPCC increases the risk of colon cancer. People with HNPCC tend to develop colorectal cancer before age 50.
- Familial adenomatous polyposis (FAP): FAP is a rare disorder in which thousands of polyps develop in the lining of your colon and rectum. These polyps then turn into cancer. People with untreated FAP have a greatly increased risk of developing colorectal cancer before age 40.
- Western diet
- Older age
- History of colorectal polyps
- Family history of colorectal cancer
- Inflammatory conditions of the colon
- Diabetes and obesity
- Smoking and alcoholism
How is rectal cancer diagnosed?
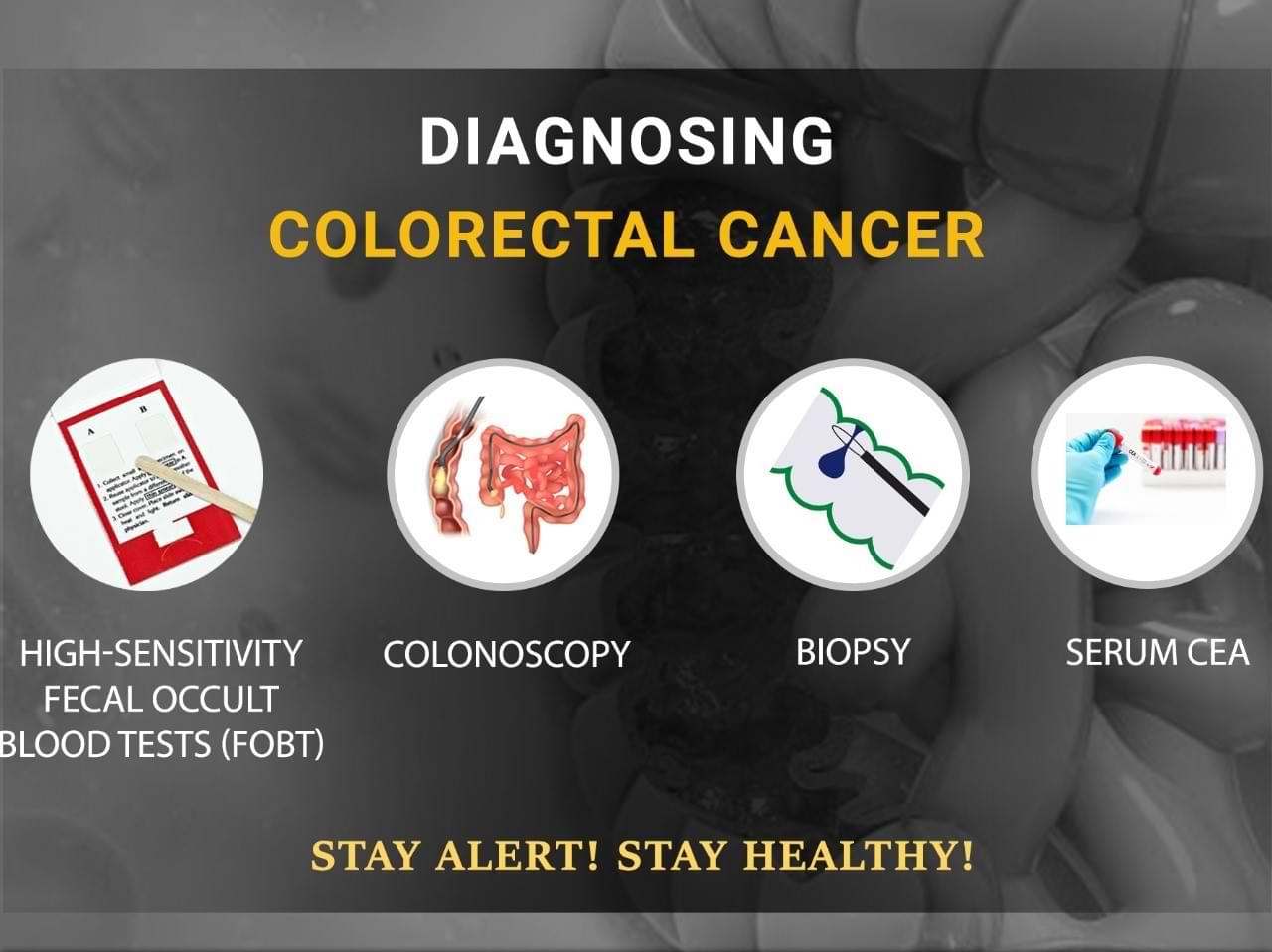
Diagnosis of colorectal cancer is established by doing a colonoscopy. It is a procedure in which a flexible thin tube with camera is passed and rectum is seen from inside. If any abnormality is seen then a small sample from it is obtained called as biopsy and examined under microscope confirming the diagnosis.
How is rectal cancer staged?
Following work-up a stage will be assigned to the tumor, which spans from I to IV. It is based on three key elements: The extent (size) of the tumor (T), The spread to nearby lymph nodes (N), and The spread (metastasis) to distant sites (M).
What is TNM staging for rectal cancer?
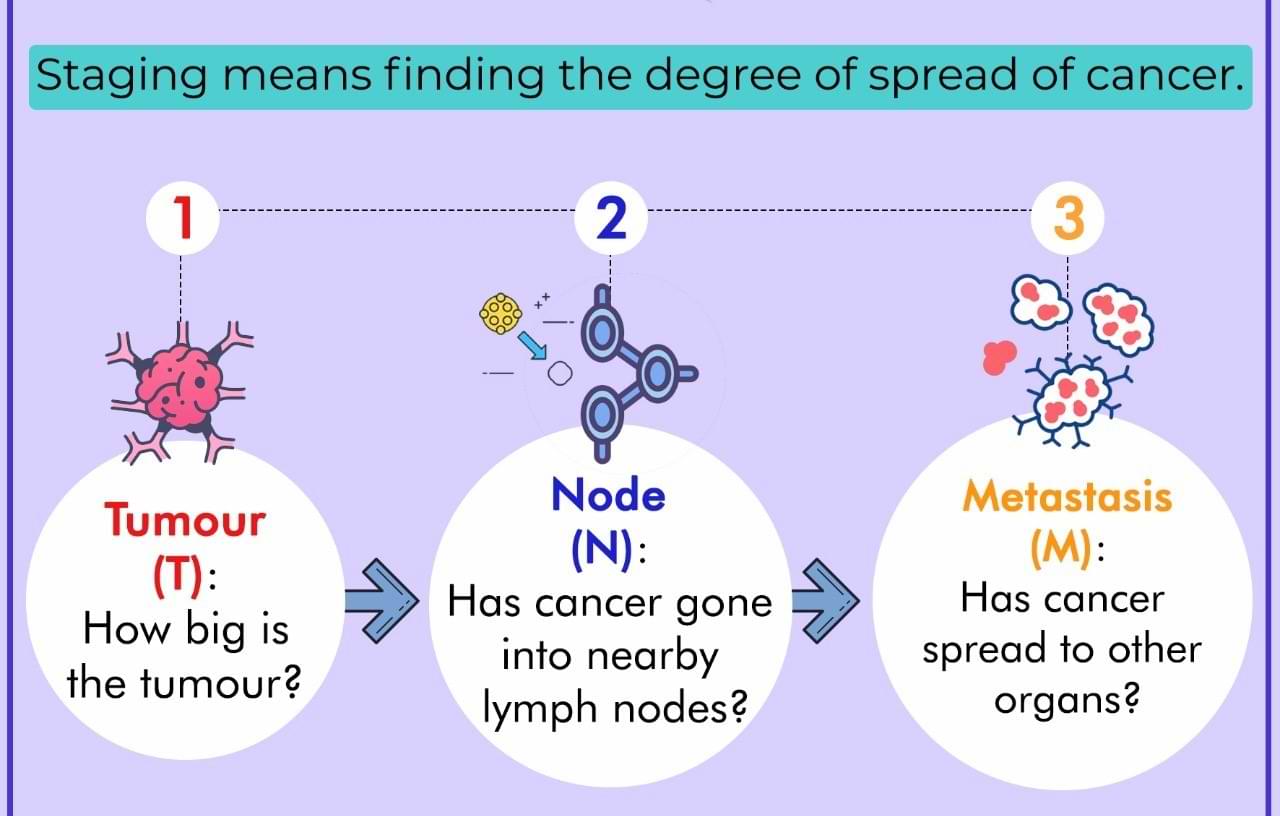
The TNM staging system is used to classify the extent of rectal cancer:
- T (Tumor): How far has the cancer grown into the layers of the rectal wall? Has the cancer reached nearby structures or organs?
- N (Node): Has the cancer spread to nearby lymph nodes? And to how many?
- M (Metastasis): Has the cancer spread to distant lymph nodes or distant organs such as the liver or lungs?
How is rectal cancer treated?
Depending upon the stage and location of the tumour in the rectum, a treatment plan is made. Surgical resection is the mainstay of treatment in those with localised disease. In early tumours surgical resection is done first and then depending upon the final stage in biopsy report, chemotherapy or chemoradiotherapy is administered.
To obtain the best results for advanced tumours chemotherapy, radiotherapy and surgery are combined in an approach called multimodal treatment. Currently, the standard of care for advanced and low rectal cancers is the administration of chemotherapy or chemoradiotherapy first called neoadjuvant treatment, followed by surgery.
How treatment is sequenced in rectal cancer?

The sequence of treatment for a rectal tumor is determined by the tumor's extent, stage, location in the rectum, the involvement of adjacent organs, fascia, and the pelvic sidewall, the presence of disease elsewhere in the body, and the proximity to the sphincter.
Radiotherapy is preferably administered before surgery and can involve either a short or long course of radiation. It is usually combined with single-agent chemotherapy. Typically, doublet chemotherapy is administered after surgery.
For very advanced tumours, both radiation and chemotherapy (or immunotherapy) are used prior to surgery to provide the best results. This approach is called total neoadjuvant treatment (TNT).
Which surgery is done for rectal cancer?
Surgery is the primary treatment for localised rectal cancer.
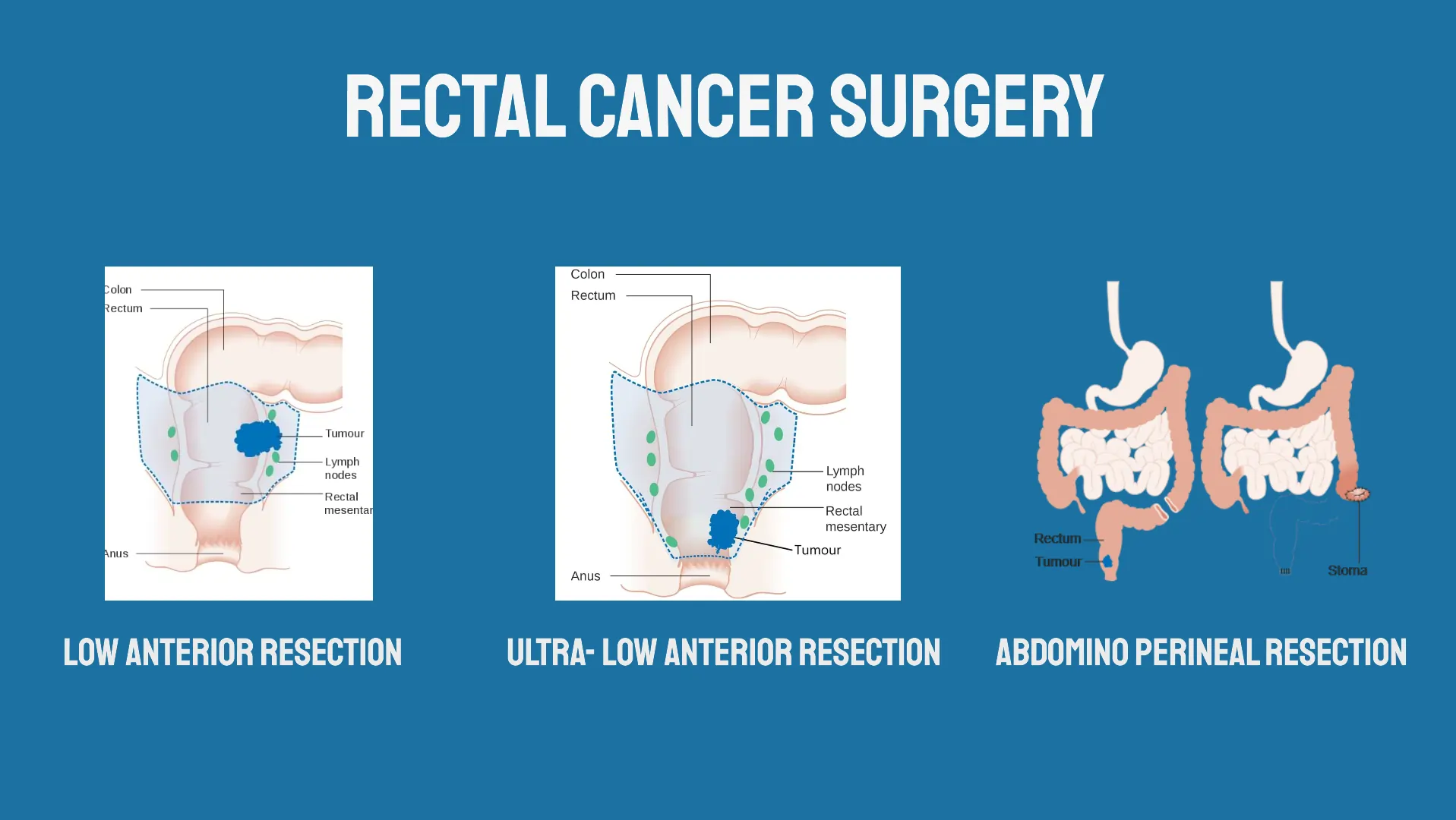
Rectal cancer surgery
- Transanal excision, transanal endoscopic microscopic surgery (TEM) and transanal minimally invasive surgery (TAMIS)
- Anterior resection and low anterior resection
- Ultra-low anterior resection, proctectomy with colo-anal anastomosis, intersphincteric resection
- Abdominoperineal resection (APR)
- Pelvic exenteration
- Total colectomy (proctocolectomy)
What are the benefits of minimally invasive surgery for rectal cancer?
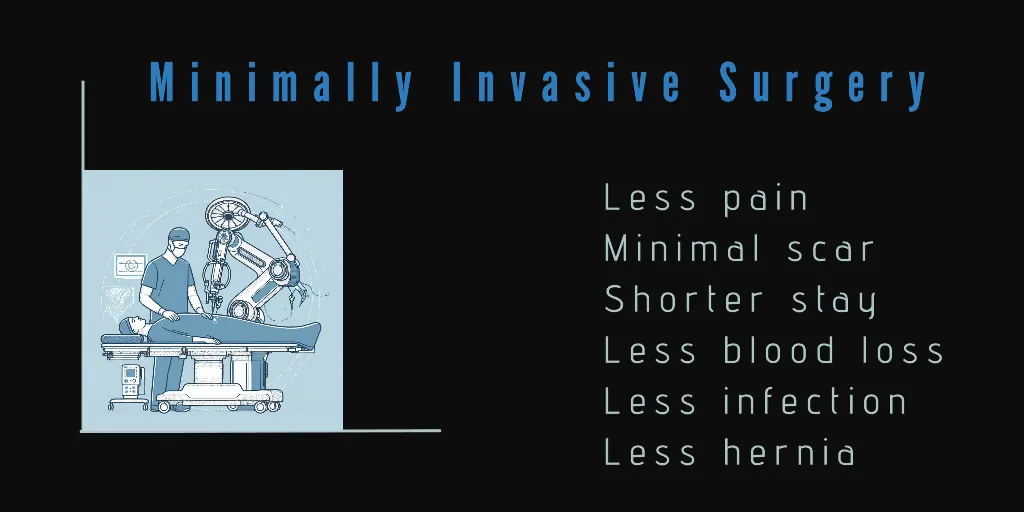
In robotic surgery or laparoscopic surgery, we make a few small holes over the abdomen.
Minimally invasive surgery is beneficial for the patient in several ways. Post-operative stress and pain are markedly reduced, leading to a faster recovery and shortened hospital/ICU stay. The amount of blood loss in the process of surgery has decreased. There is a quicker return of intestinal movement. The overall complication rate is decreased. All this results in an earlier return to home and work.
What are survival rates for rectal cancer?
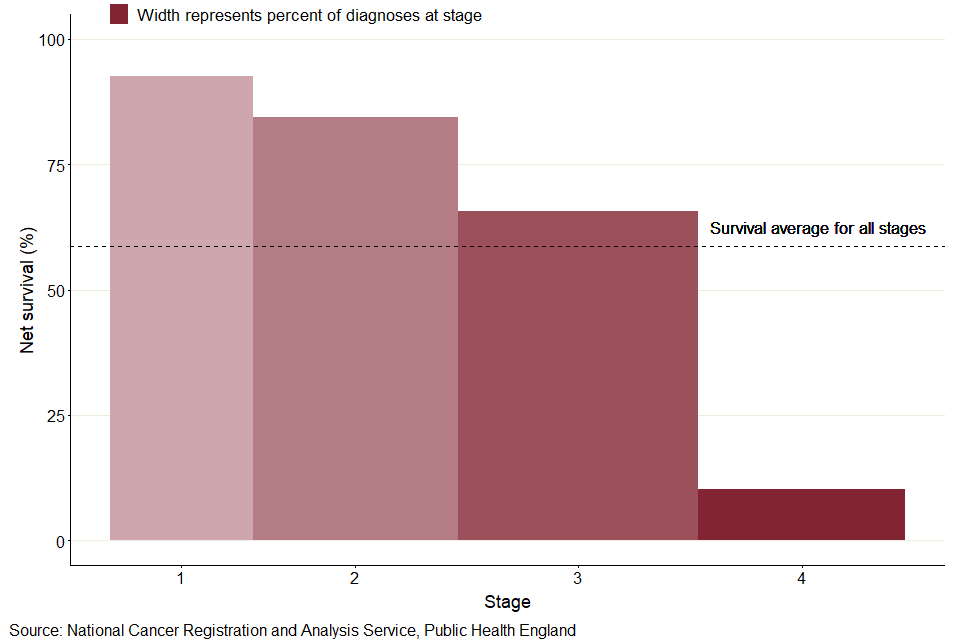
It is often measured as 5-year survival. It is the percentage of people with the same type and stage of cancer who are alive 5 years after diagnosis and they can be considered cured. These estimates are generated from many patients. After treatment for stage 1 colorectal cancer, the 5-year survival is slightly over 90%. For stage 2 it is roughly 60-90%. The 5-year survival for stage III colorectal cancer varies from 45 to 90% and for stage 4, the 5-year survival is approximately 15%.
Related topics

About Author
Dr. Nikhil Agrawal
MS, MCh
Dr. Nikhil Agrawal is a leading GI-HPB Surgical Oncologist with 20+ years of experience in complex cancers of the esophagus, stomach, colon, rectum, liver, pancreas, gallbladder, and bile ducts. He leads the GI-HPB Oncology Program at Apollo Hospitals, Delhi and Gurugram, with expertise in advanced robotic and laparoscopic cancer surgery.
His practice focuses on evidence-based, multidisciplinary care with an emphasis on individualized treatment and long-term outcomes.
He trained at BHU, SGPGI Lucknow, AIIMS New Delhi, and SNUBH, South Korea, and is a robotic surgery proctor who trains surgeons in advanced GI-HPB cancer surgery. He is also regularly invited as faculty at national and international scientific meetings.
This website helps patients and families understand GI and HPB diseases and cancers, treatment options, and what to expect during recovery and long-term care.