Periampullary Carcinoma (Periampullary Cancer)


The Ampulla of Vater
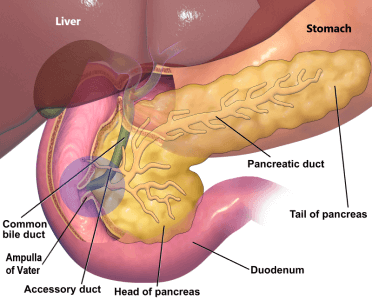
The ampulla of Vater is a mound-like opening in the duodenum. The duodenum is a C shaped loop of bowel at the beginning of the intestine. It is where the bile duct bringing bile from the liver and pancreatic duct which brings pancreatic juice from pancreas meets and then opens into the intestine.
What is periampullary cancer?
Periampullary cancer is a term used to refer to cancer that occurs in the vicinity of the ampulla of Vater. This includes cancer affecting the head of the pancreas, distal bile duct (cholangiocarcinoma), duodenum, and ampulla. It may also be called a periampullary tumour (tumor) or periampullary mass depending on clinical suspicion. These cancers are grouped together because they share similar clinical features and treatment options. Although they are all adenocarcinomas, their prognosis varies. Surgical removal of these tumors, if possible, offers the best chances of a cure.
Four Periampullary Cancer Types
- Pancreatic cancer: a cancer that originates in the pancreas.
- Distal bile duct cancer (cholangiocarcinoma): a cancer that arises from the lining of the lowermost part of the bile duct, where it passes through the pancreas, joins the pancreatic duct, and ends in the intestine.
- Duodenal cancer: a cancer that arises from the lining of the duodenal mucosa. The duodenum is the part of the small intestine where food from the stomach mixes with bile and pancreatic juice. Most duodenal cancers originate in the second part of the duodenum, where the ampulla is located.
- Ampullary cancer: a cancer that arises from the lining of the ampulla of Vater. You can read more about ampullary cancer here.
Risk factors or causes of periampullary cancer
Anything that increases your risk of getting a disease is called a risk factor. The risk of someone getting periampullary cancer increases with age. Another common risk factor is regular smoking and drinking of alcohol. Some patients get this disease because they are genetically more prone. The risk factors are slightly different for all these four cancer types.
- Pancreatic cancer: you can read about risk factors for pancreatic cancer here.
- Bile duct cancer (cholangiocarcinoma): Risk factors for bile duct cancer (cholangiocarcinoma) are infestation with some parasites such as liver flukes, primary sclerosing cholangitis, gallstones, choledochal cysts, diabetes and obesity.
- Duodenal cancer: Risk factors for duodenal cancer include inherited conditions like Familial adenomatous polyposis (FAP), Gardner syndrome, HNPCC or Lynch syndrome, juvenile polyposis syndrome and Peutz-Jeghers syndrome. Crohn's disease, celiac disease and duodenal polyps also increase the risk. Increased intake of sugar and red meat with reduced intake of fruits and vegetables has also been incriminated.
- Ampullary cancer: Risk factors for ampullary cancer have not been defined due to the low incidence of this disease in the population. According to a case-control study, previous cholecystectomy (gallbladder removal) and use of proton pump inhibitors (PPIs) were associated with increased risk of ampullary tumors.
Signs and symptoms of periampullary cancer
Periampullary cancers compress the bile duct, blocks the flow of bile and cause yellowing of eyes and urine called jaundice. This is usually accompanied by pale stools and itching. Other warning signs of periampullary cancer can be weight loss, loss of appetite and abdominal pain. Besides, duodenal and ampullary cancers bleed causing black stools (melena) and anaemia.
Signs and symptoms of periampullary cancer
- Jaundice (yellowing of skin, eyes and urine with pale stools)
- Itching
- Abdominal pain
- Weight loss and loss of appetite
- Recurrent vomiting
- Black stools
- Anaemia
Diagnosis and staging of periampullary cancer
Once a periampullary mass, growth, or tumour is suspected, it is diagnosed and staged using either a high-resolution, thin-cut, triple-phase CT scan of the abdomen combined with a CT scan of the chest, or a PET-CT scan. We prefer to perform a high-resolution, thin-cut PET-CT with a dedicated triple-phase contrast-enhanced CT protocol, which accurately evaluates the local tumour extent and detects distant metastases. Your surgeon will also do tests to quantify your jaundice, check your kidney function, haemoglobin and blood clotting parameters. A tumour marker called CA19.9 will also be checked.
Additional investigations may be required to confirm the diagnosis, accurately stage the disease, and plan the most appropriate treatment. Depending on the clinical situation, these may include the following:
- Side viewing endoscopy: it is a procedure in which a thin flexible tube is passed into your intestine through your mouth. It has a camera at the tip of the tube and a view of the ampulla is obtained, showing any periampullary growth.
- Biopsy: if a tumour is found at the ampulla, then a small sample from it is obtained called as biopsy and examined under microscope confirming the diagnosis.
- Endoscopic ultrasound (EUS): it is like doing an ultrasound of the periampullary region from the inside of your intestine. It aids diagnosis in cases where CT/MRI do not show cancerous growth, while it is suspected on clinical features. It is also used to take a sample from the tumour by passing a needle called fine needle aspiration cytology (FNAC) for confirmation of diagnosis if required.
Staging is based on the TNM classification and determines whether the cancer is localized, locally advanced or metastatic. Accurate staging helps decide whether surgery, chemotherapy or both are required.
Treatment of periampullary cancer
Treatment depends on the stage of the disease, the degree of jaundice, and the patient's overall fitness. Every patient is discussed in a multidisciplinary team (MDT) meeting to determine the most appropriate treatment strategy. Surgery (Whipple procedure or pancreaticoduodenectomy) offers the best chance of cure and is recommended when the cancer can be completely removed.
If jaundice is severe, your surgeon may advise endoscopic retrograde cholangiopancreatography (ERCP) with stenting before surgery. During this procedure, a plastic or metallic stent is placed across the blocked bile duct to relieve jaundice and improve liver function before definitive treatment.
For patients with borderline resectable or locally advanced disease, neoadjuvant treatment (chemotherapy with or without radiotherapy) may be recommended after reducing jaundice to shrink the tumour, improve the likelihood of complete surgical removal, and achieve better long-term outcomes. In some cases, this approach can downstage the disease sufficiently to make curative surgery possible.
Patients with metastatic disease are usually treated with palliative systemic therapy, supportive care, and metallic stenting to relieve jaundice and improve quality of life.
Surgery for periampullary cancer
The operation performed to remove periampullary cancer is called the Whipple procedure, also known as pancreaticoduodenectomy. It is a complex and major abdominal surgery that involves careful dissection around important blood vessels near the pancreas and is typically performed in specialised centres by experienced surgical teams. During this operation, the head of the pancreas, duodenum, distal bile duct, gallbladder, part of the stomach (in a standard Whipple procedure), a small segment of the small intestine, and the adjacent lymph nodes are removed. The aim of the surgery is to completely remove the tumour along with surrounding tissues that may contain microscopic disease, thereby offering the best chance of long-term survival.
The digestive tract is then reconstructed by joining the remaining pancreas, bile duct, and stomach (or duodenum in selected patients undergoing a pylorus-preserving pancreaticoduodenectomy) to the small intestine. This is done through pancreaticojejunostomy (PJ), where the pancreas is connected to the small intestine, or pancreaticogastrostomy (PG), where the pancreas is connected to the stomach; hepaticojejunostomy (HJ), where the bile duct is connected to the small intestine; and gastrojejunostomy (GJ), where the stomach is connected to the small intestine, allowing normal digestion to continue.
In appropriately selected patients, the Whipple procedure can be performed using minimally invasive techniques, including laparoscopic or robotic surgery. We prefer the robotic Whipple approach because of its advantages. Robotic Whipple uses advanced systems that provide the surgeon with a clear 3D view and enhanced dexterity through wristed instruments that allow 360-degree movement, filter hand tremors, and stabilize movements for precise dissection, enabling more accurate surgery. This helps reduce blood loss and complications. Minimally invasive approaches are associated with smaller incisions, reduced postoperative pain, shorter hospital stays, and faster recovery, while maintaining comparable oncological outcomes when performed in experienced centres.
Palliative treatment
For patients with cancer that has spread to other parts of the body (metastatic periampullary cancer), the aim of treatment is to relieve symptoms, maintain quality of life, and prolong survival. Systemic chemotherapy is the main treatment and is usually started after confirmation of the diagnosis by biopsy. In addition, molecular profiling using next-generation sequencing (NGS) is increasingly recommended to identify actionable genetic alterations. This can help guide the use of targeted therapies and immunotherapy in selected patients, such as those with specific mutations or biomarkers (e.g., MSI-high/dMMR, HER2 amplification, or other targetable alterations), offering a more personalized treatment approach.
If obstructive jaundice is present, biliary drainage is performed before chemotherapy, usually by endoscopic retrograde cholangiopancreatography (ERCP), during which a plastic or self-expanding metallic stent is placed across the blocked bile duct to relieve jaundice, improve liver function, and reduce symptoms such as itching, thereby helping patients become fit to receive chemotherapy. In cases where ERCP is not feasible or unsuccessful, percutaneous transhepatic biliary drainage (PTBD) may be required.
If the tumour causes gastric outlet obstruction and prevents food from passing normally, an endoscopic duodenal stent may be inserted to restore oral intake. Endoscopic gastrojejunostomy (EUS-guided GJ) is another minimally invasive option to bypass the obstruction. If endoscopic methods are not feasible or unsuccessful, a surgical bypass may be required.
Prognosis (survival rate) of periampullary cancer
It is often measured as 5-year survival. It is the percentage of people with the same type and stage of cancer who are alive 5 years after diagnosis. These estimates are generated from many patients. The overall long-term survival rate for ampullary and duodenal carcinoma after the Whipple procedure is 55-60%. For pancreatic cancer and distal cholangiocarcinoma, the overall long-term survival rate after surgery is 35-45%.
Frequently Asked Questions
Detect Early, Treat Right, Save Lives!

About Author
Dr. Nikhil Agrawal
MS, MCh
Dr. Nikhil Agrawal is a leading GI-HPB Surgical Oncologist with 20+ years of experience in complex cancers of the esophagus, stomach, colon, rectum, liver, pancreas, gallbladder, and bile ducts. He leads the GI-HPB Oncology Program at Apollo Hospitals, Delhi and Gurugram, with expertise in advanced robotic and laparoscopic cancer surgery.
His practice focuses on evidence-based, multidisciplinary care with an emphasis on individualized treatment and long-term outcomes.
He trained at BHU, SGPGI Lucknow, AIIMS New Delhi, and SNUBH, South Korea, and is a robotic surgery proctor who trains surgeons in advanced GI-HPB cancer surgery. He is also regularly invited as faculty at national and international scientific meetings.
This website helps patients and families understand GI and HPB diseases and cancers, treatment options, and what to expect during recovery and long-term care.