Surgery for Rectal Cancer


Understanding the approach
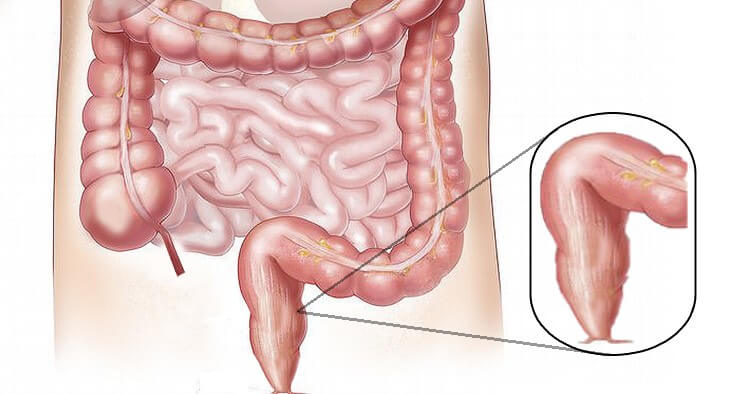
The rectum is the last part of the intestine and ends in the anal opening. The treatment of rectal cancer depends on the stage and local extent of the disease. Surgery is the primary treatment for earlier stage rectal cancer. Radiation and chemotherapy are given before surgery in advanced rectal cancers.
When a surgeon operates for cancer, he removes the cancer-bearing organ or part of it to the healthy tissue along with the adjacent draining lymph nodes. Lymph nodes are small glands that are part of our lymphatic system. They are situated alongside the blood vessels that supply blood to the concerned organ. Lymph nodes play a vital role in our body's defence system. They filter and trap the cancer cells, preventing them from reaching other organs of our body (metastasis).
Lymph nodes are situated along the blood vessels and in the mesorectum.
Rectal cancer surgery
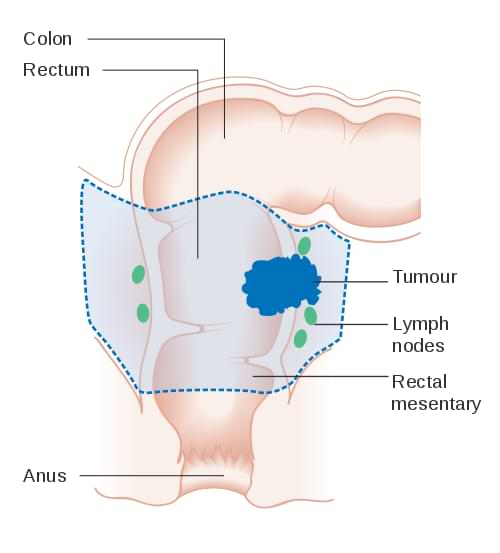
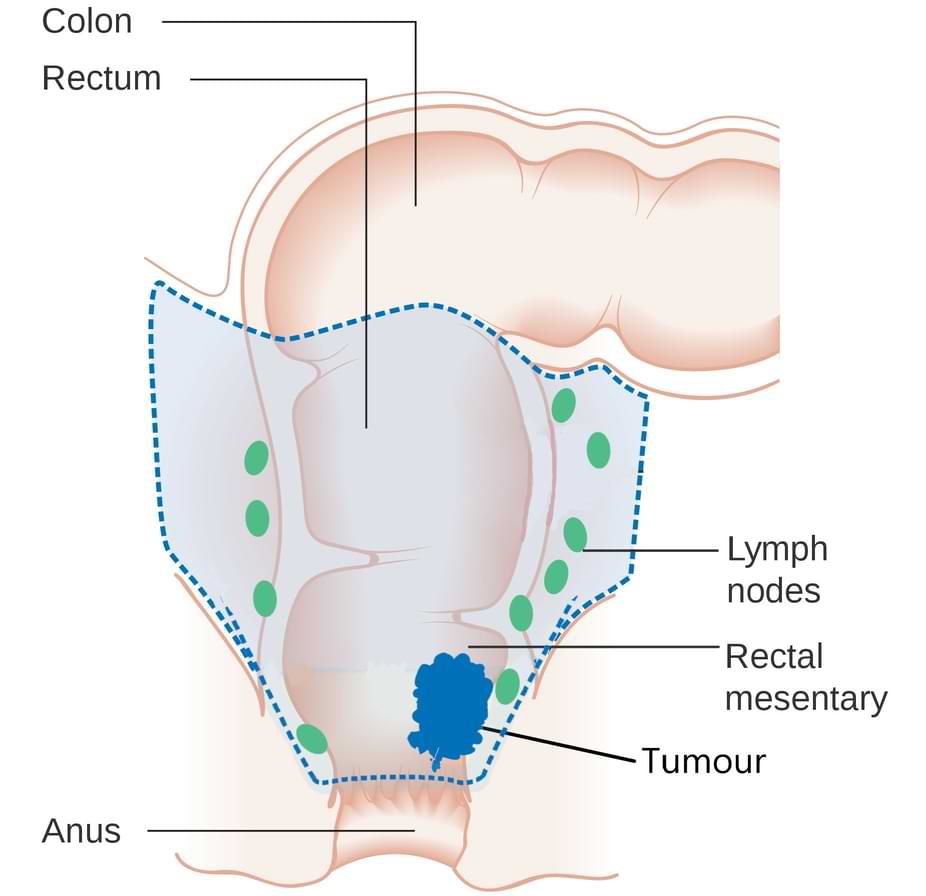
The type of surgery depends on the location and extent of cancer in the rectum. The relationship of the tumour to the anus is essential in determining the type of surgery. If the cancer is infiltrating the anal sphincter then it is also removed.
The surgical procedure to remove the whole or part of the rectum is given various names depending on the extent of colon and rectum resected. These are local excision, anterior resection, low anterior resection, ultra-low anterior resection, intersphincteric resection, abdominoperineal resection and pelvic exenteration.
If we can preserve the lower end of the rectum or anus then the cut ends are reattached. This allows the patient to keep anal function and pass stools in a normal manner.
If this attachment is not healthy or too close to the anal canal, then a diverting ileostomy is done, in which a loop of the small intestine is brought out onto the abdomen. Sometimes we can not spare the anus. Then, we make a permanent colostomy. The stool is collected into a bag that fits securely over the abdominal wall around the opening.
Local resection
Transanal excision, Transanal endoscopic microsurgery (TEM), Endoscopic submucosal dissection (ESD), Transanal minimally invasive surgery (TAMIS)
Very early cancer that is limited to the inner layer of the rectum without lymph nodal involvement can be removed with these approaches. In these techniques, the tumour is approached and resected by instruments inserted through the anal opening.
Anterior resection and low anterior resection
For upper and middle rectal cancers, the tumour-bearing part of the rectum is removed with a healthy margin and lymph nodes. The colon is then reattached to the remaining rectum. The rectum is wrapped in a tissue called the mesorectum. It is important to include it in the resection, a technique called total mesorectal excision (TME).
Rectal cancer surgery | Low anterior resection
Ultra-low anterior resection, Intersphincteric resection
These operations are done for tumours involving the lowest part of the rectum, just above the anal canal (or, part of the inner layer of the anal sphincter). In these operations, the entire rectum is removed and the colon is attached to the upper part of the anal canal. Sometimes the inner layer of the anal sphincter is also partially removed, called intersphincteric resection.
Rectal cancer surgery | Ultra-low anterior resection
Abdominoperineal resection (APR)
When cancers of the lower rectum involve the muscles of the anal canal (anal sphincters), the anal canal needs excision. As the anus is removed, a permanent colostomy is created.

Rectal cancer surgery | Abdominoperineal resection
Pelvic exenteration
Some rectal cancer grows into nearby organs. This includes the urinary system in front of the rectum. The surgery in such cases will also remove part of the urinary system. This procedure is called pelvic exenteration.
Total colectomy (proctocolectomy)
Sometimes, the whole colon needs to be removed along with the rectum. It is called total colectomy or proctocolectomy.
This procedure is done when multiple polyps, inflammatory bowel disease or dilatation because of intestinal obstruction affects the large intestine.
There are two ways to do rectal cancer surgery:
- Open
- Minimally Invasive (laparoscopic or robotic)
Open surgery
In open surgery, we make a single long incision over the abdomen to do the surgery. This was the traditional way of doing the surgery. It resulted in delayed recovery, long hospital stays and nasty scars.
Minimally invasive rectal cancer surgery
Laparoscopic rectal cancer surgery
Laparoscopic, or keyhole surgery minimizes suffering and improves outcomes. It has now become a standard for most gastrointestinal operations.
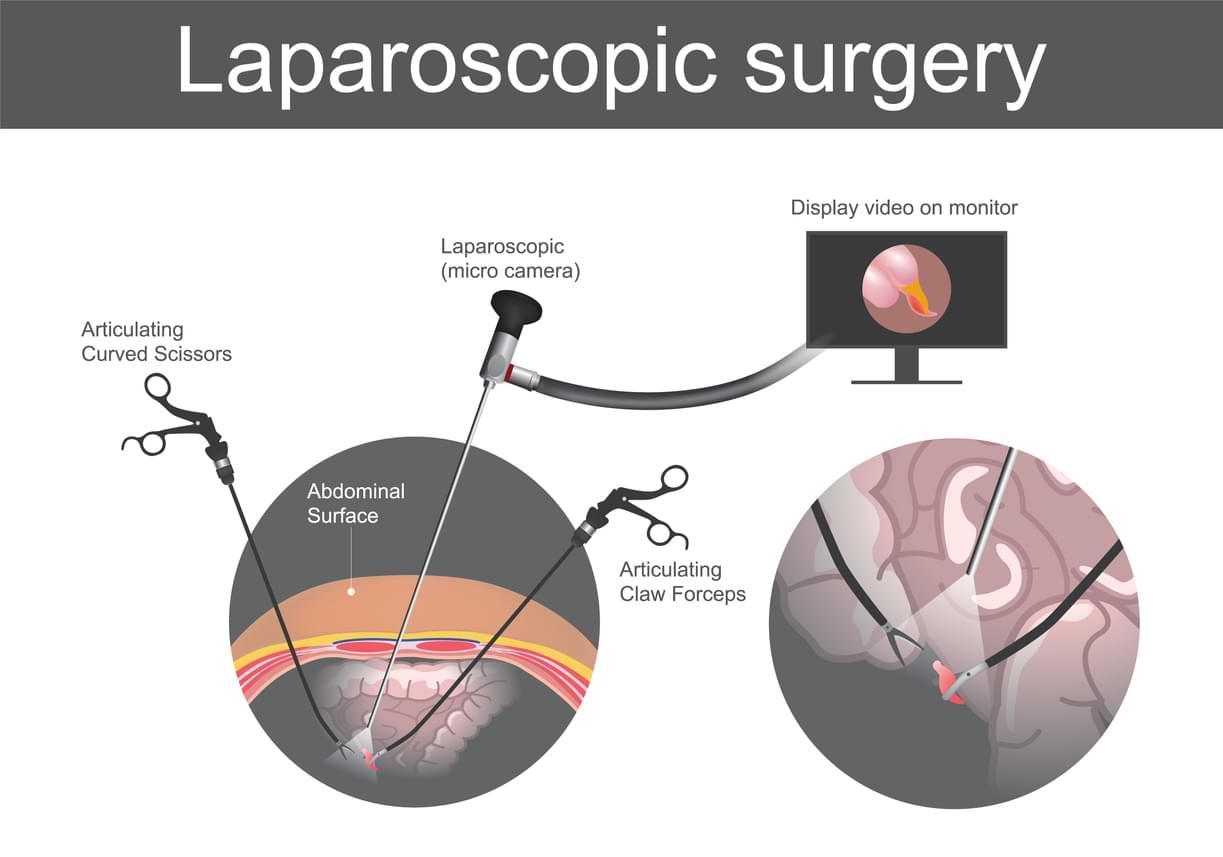
In laparoscopic surgery, we make a few small holes called ports over the abdomen. One of them is used to insert a slender high-resolution camera that projects a magnified view of the inside of the abdomen onto a high definition monitor. The rest of the ports are used for long and thin instruments. The surgeon deftly manoeuvres the instruments looking at the monitor.
Robotic rectal cancer surgery
Robotic surgery combines the skill and expertise of a surgeon with the vision, precision, and flexibility of robotic technology. The robotic system features a 3D high-definition camera system for clear and enhanced vision with depth perception. It comprises a surgical console, where the surgeon sits, and robotic arms equipped with surgical instruments. The tiny wristed instruments can bend and rotate in ways the human hand cannot, allowing the surgeon to operate in tight spaces.
During robotic surgery, the surgeon makes minor cuts in the abdomen and inserts special tubes called ports. The robotic arms are connected to these ports, and the instruments mounted on these robotic arms go through the ports to do the surgery. A slender camera is also inserted through one port to show the surgeon a clear view of the inside. The surgeon controls the robotic arms from a console nearby, and an assistant helps by changing the instruments and aiding as needed.
Benefits of robotic and laparoscopic rectal cancer surgery
Minimally invasive surgery is beneficial for the patient in several ways. Post-operative stress and pain are markedly reduced, leading to a faster recovery and shortened hospital/ICU stay. The amount of blood loss in the process of surgery has decreased. There is a quicker return of intestinal movement. The overall complication rate is decreased. All this results in an earlier return to home and work. The absence of a long scar is pleasant to the eyes.
Rectal cancer and intestinal obstruction
Cancer will sometimes block the rectum, a condition called intestinal obstruction. In such cases, a colostomy is made before starting the radiotherapy and chemotherapy. In some cases and in those where curative surgery is not an option, a stent can be placed to relieve the obstruction.
Treatment of advanced (stage 4) rectal cancer
Many rectal cancer patients will have stage 4 cancer at the time of presentation. Stage 4 cancer means that rectal cancer has spread to other organs of the body.
Metastatic GI cancers are generally considered incurable. However, in rectal cancer, if cancer has spread only to a few spots in the liver, lung or peritoneum then surgery can be used to remove them completely. In some of these cases, we prefer to give chemotherapy (along with radiation) first and then do the surgery. This approach helps the patients live longer and provides them with a chance to be free of cancer over the long term.
Liver resection
It is a surgical procedure to remove cancer containing part of the liver, also called hepatectomy or metastasectomy.
Lung resection
Pulmonary (lung) resection is a surgical procedure to remove the part of the lung, which has cancer.
Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC)
Cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (HIPEC) treats colorectal cancers that have a limited spread to the abdominal cavity (peritoneum). During cytoreductive surgery, all visible tumours are surgically removed, which only leaves microscopic cancer cells. Cytoreductive surgery is followed by HIPEC, which aims to destroy the remaining microscopic cancer cells. In HIPEC, concentrated and heated chemotherapy solution is delivered directly into the abdominal cavity, which kills those cells.
This approach helps the patients live longer and provides them with a chance to be free of cancer over the long term.
Risks (complications) of rectal cancer surgery
All surgeries can be associated with complications and so is the case with rectal cancer surgery. Some common possible complications after rectal cancer surgery include:
- Anastomotic leak: the joint of the intestine can leak.
- Infections - surgical site, pulmonary: Infections can occur after the surgery.
- Cardiac complication: Heart-related complications
- Bleeding: There can be bleeding during or after surgery
- Injury to adjacent organs: Many internal organs are very close to the colon and rectum. They can be injured during surgery. This can affect urinary and sexual function.
- Anaesthesia related complications: There can be complications related to the administration of anaesthesia and recovery.
- Postoperative obstruction: Post-surgery intestines can stop working, a condition known as postoperative ileus. They can get stuck or entangled, requiring surgery.
- Deep venous thrombosis: Clots can form in the veins of the leg due to immobility. These clots can travel to the lung also.
- Hernia: Hernia can form at the incision site.
- Increased stool frequency
Before surgery
The following steps will be taken to ensure the best outcome.
- Tests related to diagnosis, staging and surgical planning
- Tests related to fitness for surgery
- Optimising coexisting illness: Those with pre-existing illnesses such as diabetes, hypertension, cardiac disease etc. will be optimised to the best possible health.
- Admission and bowel preparation: Some patients will be given medicine to empty the colon before the surgery.
- Can read more about preparing for surgery here.
After surgery
You will be closely monitored while you recover. It generally goes through the following steps.
- Intensive monitoring: Monitoring takes place in the ICU or recovery room
- Removal of tubes (Nasogastric, Foley and drain): Few tubes are placed during the surgery to facilitate the recovery. They are removed sequentially.
- Start and increase the diet: The oral intake is started with clear fluids and increased to a liquid diet and soft diet over a few days.
- Discharge: Once you are fully mobile and oral intake is adequate you will be discharged with instructions to follow at home. This usually happens 4-6 days after surgery.
- Follow-up: A follow-up visit is planned a week or 10 days after discharge. Clips or stitches over the incision are removed. The final biopsy report and further treatment plans are discussed.
Detect Early, Treat Right, Save Lives!

About Author
Dr. Nikhil Agrawal
MS, MCh
Dr. Nikhil Agrawal is a leading GI-HPB Surgical Oncologist with 20+ years of experience in complex cancers of the esophagus, stomach, colon, rectum, liver, pancreas, gallbladder, and bile ducts. He leads the GI-HPB Oncology Program at Apollo Hospitals, Delhi and Gurugram, with expertise in advanced robotic and laparoscopic cancer surgery.
His practice focuses on evidence-based, multidisciplinary care with an emphasis on individualized treatment and long-term outcomes.
He trained at BHU, SGPGI Lucknow, AIIMS New Delhi, and SNUBH, South Korea, and is a robotic surgery proctor who trains surgeons in advanced GI-HPB cancer surgery. He is also regularly invited as faculty at national and international scientific meetings.
This website helps patients and families understand GI and HPB diseases and cancers, treatment options, and what to expect during recovery and long-term care.