Stomach Cancer



Overview
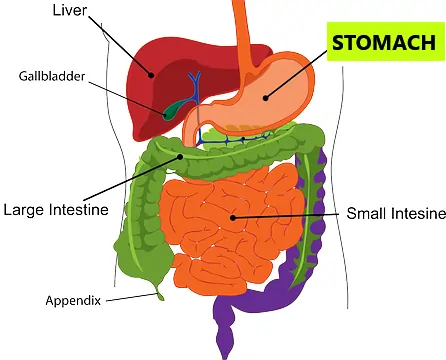
After swallowing, food passes through the oesophagus (food pipe) and then enters a sac-like organ in the upper abdomen called the stomach. The stomach holds food and starts to digest it by secreting gastric juice. The stomach empties food mixed with gastric juice into the first part of the small intestine called the duodenum.
Cancer begins when an error (mutation) occurs in a cell's DNA. The cells then divide and grow uncontrolled. These accumulated cells form cancer. The stomach wall is made of five layers of tissue. Stomach cancer, also called gastric cancer, begins in the innermost layer, mucus-producing cells that line the stomach. It then advances and spreads.
Stomach cancer is the 5th most commonly diagnosed cancer in the world. Over 10 lakh cases of gastric cancer are diagnosed each year around the world.
Types of stomach cancer
- Adenocarcinoma; it is the most common subtype (90-95%)
- Gastrointestinal stromal tumour (GIST)
- Neuroendocrine tumours (NET)
- Lymphoma
Risk factors for stomach cancer
Anything that increases the risk of someone getting cancer is a risk factor. The risk factor does not directly cause the disease. Some with many risk factors will not get the disease, while some with no known risk factor will get it.
Risk factors for stomach cancer are:
- Older age
- Male gender
- Infection with a bacterium called H. pylori
- Persistent inflammation called gastritis
- Pernicious anaemia
- Certain types of polyps in the stomach
- Smoking
- Obesity
- Diet high in smoked, pickled or salty foods
- Diet deficient in fruits and vegetables
- Family history of stomach cancer
- Inherited cancer syndromes
Symptoms of stomach cancer
While stomach cancer is relatively rare compared to other types of cancer, one of the biggest dangers of this disease is the difficulty of diagnosing it. Gastric cancer like most gastrointestinal cancers is asymptomatic in initial stages. It often goes undiagnosed until after it spreads to other parts of the body. This makes it difficult to treat.
The symptoms, if occur, include:
- Indigestion, heartburn, and bloating
- Loss of appetite
- Unexplained weight loss
- Early satiety (feeling full after eating only a small amount of food)
- Bloody or black stool
- Abdominal pain, which may be worse after meals
- Nausea and vomiting, with or without blood
- Vague discomfort in the upper abdomen
- Low haemoglobin (anaemia)
- Fatigue
Diagnosis of stomach cancer
Physical history and examination
Understanding symptoms and checking for signs by a physician are basics of arriving at a diagnosis.
Upper GI endoscopy
Upper endoscopy establishes the diagnosis of stomach cancer. It is a procedure in which a flexible thin tube with a camera sees the stomach from inside.
Biopsy
On endoscopic examination any abnormality is sampled and examined under microscope confirming the diagnosis.
Determining the extent of disease (staging)
The cancer cells break away from the primary tumour and spread through the body in one of the three ways; a) bloodstream, b) lymphatic system or c) directly through the tissue.
The spread could be; local, through the layers of the stomach, to the adjacent lymph nodes and the nearby organs. Or, the spread could be distant, to the liver, lungs and the peritoneal lining of the abdomen. The distant spread is metastasis.
Staging is finding out the extent of the disease. After the diagnosis of stomach cancer, we do tests to find out how much the tumour has spread. Depending upon the suspected extent of disease some of the following investigations will be done to determine the exact stage.
- Blood tests: Complete blood count measures the distinct types of cells in the blood. Some patients have low haemoglobin (anaemia). Besides, liver and kidney function tests assess the function of these organs.
- Computed tomography (CT) scan: CT Scanner acquires images of the inside of our body with the help of x-ray beams. These images are then computer-processed giving an accurate representation. Contrast injected into the blood enhances these images.
- Positron emission tomography (PET) scan: Cancer cells take up a larger amount of glucose. Here injected radioactive glucose (18F-fluorodeoxyglucose; FDG) binds to the tumour, and the patient is scanned. The images are computer-processed and combined with CT images, giving us a CT image with bright tumours.
- Endoscopic ultrasound (EUS): It is an ultrasound of the stomach from inside. It is useful in small tumours. It sees how far cancer has spread into the layers of the stomach and the adjacent lymph nodes.
- Laparoscopy: CT and PET scans can miss small tumours. In laparoscopy, a slender camera is inserted through a small hole in your abdomen and small deposits over the liver and peritoneal lining can be detected. It is usually done before giving neoadjuvant chemotherapy and surgery.
This work-up will help us assign a stage to the tumour, broadly classifying them into:
- Localised - Tumour is limited to the organ in which it started.
- Regional spread - The tumour has spread to nearby lymph nodes and/or has come out of the wall of the organ in which it started.
- Distant spread - The tumour has spread to organs, which are away from the organ of origin of the tumour, called metastasis.
TNM (tumour, node and metastasis) classification
- The extent (size) of the tumour (T): How far has cancer grown into the 5 layers of the stomach wall? Has cancer reached nearby structures or organs?
- The spread to nearby lymph nodes (N): Has cancer spread to nearby lymph nodes? And to how many?
- The spread (metastasis) to distant sites (M): Has cancer spread to distant lymph nodes or distant organs such as the liver or lungs?
Numbers and letters after T, N and M give further details. Higher the number, more advanced the tumour. Combined Information from T, N and M assigns an overall stage, a process called stage grouping. Stomach cancer stage ranges from I to IV. Stages I to III are localized disease and stage IV is advanced cancer (metastatic disease). Chances of recovery from cancer (prognosis) depend on the stage of the disease at the time of diagnosis. Lower the stage, better is the long-term prognosis.
The definite stage is determined after surgery by histopathological examination of the removed cancer specimen. It is called surgical staging. The stage determined after imaging tests is the clinical stage.
Treatment of stomach cancer
Treatment will depend upon the stage of tumour and fitness of the patient to undergo a major surgical procedure. Treatment can be broadly categorised into curative and palliative.
Curative treatment aims to eradicate the disease. To get the best results in advanced tumours, chemotherapy and/or radiotherapy and surgery are combined in an approach called multimodal treatment. Depending upon the extent of tumour, chemotherapy or chemoradiation can be given before surgery or after surgery.
Surgery for stomach cancer:
Treatment of localized disease
Radical gastrectomy (subtotal and total)
Surgery is the primary treatment for earlier stage stomach cancer. It entails the removal of the diseased stomach with a margin of healthy tissue, omentum and adjacent lymph nodes. Intestinal continuity is then re-established by joining the ends of the stomach with the small intestine (anastomosis).
There are two ways to do a gastrectomy:
- Open, and
- Laparoscopic or Robotic
In open surgery, a single long incision is made over the abdomen to do the surgery.
Laparoscopic stomach cancer surgery
The laparoscopic approach uses minimally invasive techniques to do the same surgery with tiny incisions. This entails the insertion of special long thin surgical tools through these small holes. This results in faster recovery and reduced pain compared to conventional open surgery. This requires expertise. Make sure your surgeon is skilled and has done many of these operations.
Robotic surgery for stomach cancer
Robotic surgery combines the skill and expertise of a surgeon with the vision, precision, and flexibility of robotic technology. The robotic system features a 3D high-definition camera system for clear and enhanced vision with depth perception. It comprises a surgical console, where the surgeon sits, and robotic arms equipped with surgical instruments. The tiny wristed instruments can bend and rotate in ways the human hand cannot, allowing the surgeon to operate in tight spaces.
During stomach cancer surgery, the surgeon makes minor cuts in the abdomen and inserts special tubes called ports. The robotic arms are connected to these ports, and the instruments mounted on these robotic arms go through the ports to do the surgery. A slender camera is also inserted through one port to show the surgeon a clear view of the inside. The surgeon controls the robotic arms from a console nearby, and an assistant helps by changing the instruments and aiding as needed.
Treatment of advanced cancer
Chemotherapy
Chemotherapy uses drugs to destroy cancer cells. Several drugs are combined and given in a specific order on specific days as cycles.
- Adjuvant chemo - In patients with localized stomach cancer, chemotherapy is usually given after surgery to kill the cells which could remain. The decision to give chemotherapy depends on the surgical stage. It is usually administered if cancer has spread to lymph nodes or penetrated outer layers of the stomach. In this way, chemotherapy helps reduce the risk of cancer recurrence and death from cancer.
- Neoadjuvant chemo - If the tumour has excessively grown, then chemotherapy is administered before surgery. It will shrink cancer and produce a better result from an operation later.
- Palliative chemo - In metastatic cancers, chemotherapy prolongs survival and improves the quality of life.
Targeted therapy
Substances which identify and attack cancer cells without harming normal cells. Targeted therapy for stomach cancer includes HER2-targeted therapy and Anti-angiogenesis therapy.
Immunotherapy
It uses the patient's immune system to fight cancer. Immune checkpoint inhibitor therapy is a type of immunotherapy.
Radiation therapy
Radiation therapy uses high energy X-rays to destroy cancer cells. People with stomach cancer usually receive external-beam radiation therapy, which is radiation given from a machine outside the body. Radiation therapy may be used before surgery to shrink the size of the tumour or after surgery to destroy any remaining cancer cells.
Palliative treatment
Palliative treatment relieves symptoms and improves the quality of life. It is considered when the tumour is too advanced or disseminated. A patient unfit for major surgery is also treated with palliative intent. Blockage in the stomach can be treated by inserting a stent (a hollow metal tube). Chemotherapy can provide symptomatic relief along with prolonging life. Sometimes surgery such as gastrojejunostomy or gastrectomy is also needed for symptoms or complications.
Prognosis
Survival rates
According to the American Cancer Society, the percentages of people who live for at least five years after being diagnosed with stomach cancer is 68-82% for stage II and 18-54% for stage III cancers.
Prevention of stomach cancer
We can categorise the risk factors for stomach cancer into modifiable and non-modifiable. Age and genetic factors are non-modifiable, and we can't do anything about it. However, we can decrease our risk of getting stomach cancer by modifying our behaviour.
We can lower our risk by taking the following steps:
- Regular physical activity and exercise
- Maintain a healthy weight
- Eat a healthy diet rich in fruits, vegetables and whole grains
- Reduce the intake of salty and smoked foods
- Avoid tobacco and smoking
- Limit alcohol intake
- Treating H pylori infection
Detect Early, Treat Right, Save Lives!

About Author
Dr. Nikhil Agrawal
MS, MCh
Dr. Nikhil Agrawal is a leading GI-HPB Surgical Oncologist with 20+ years of experience in complex cancers of the esophagus, stomach, colon, rectum, liver, pancreas, gallbladder, and bile ducts. He leads the GI-HPB Oncology Program at Apollo Hospitals, Delhi and Gurugram, with expertise in advanced robotic and laparoscopic cancer surgery.
His practice focuses on evidence-based, multidisciplinary care with an emphasis on individualized treatment and long-term outcomes.
He trained at BHU, SGPGI Lucknow, AIIMS New Delhi, and SNUBH, South Korea, and is a robotic surgery proctor who trains surgeons in advanced GI-HPB cancer surgery. He is also regularly invited as faculty at national and international scientific meetings.
This website helps patients and families understand GI and HPB diseases and cancers, treatment options, and what to expect during recovery and long-term care.