Surgery (Radical Cholecystectomy) for Gallbladder Cancer Treatment
The gallbladder and its location in the body


Gallbladder Cancer
Cancer forms when healthy cells develop changes (mutations) in their DNA. These cells begin to grow uncontrolled, don't die and forms a growing clump called tumour or cancer. Gallbladder cancer begins in the inner layers of the gallbladder. It gradually grows beyond the gallbladder wall and spreads to the liver, bile duct, adjacent lymph nodes and other areas of the body.
Surgical principles
The gallbladder is a pear-shaped organ underneath your liver. Liver and gallbladder are behind the ribs in the right upper abdomen. The treatment of gallbladder cancer depends on the stage and local spread of the disease. Surgery is the primary treatment for earlier stage gallbladder cancer.
When a surgeon operates for cancer, he removes the cancer-bearing organ or part of it to the healthy tissue along with the adjacent draining lymph nodes.
Lymph nodes are small glands that are part of our lymphatic system. They are situated alongside the blood vessels that supply blood to the concerned organ. Lymph nodes play a vital role in our body's defence system. They filter and trap the cancer cells, preventing them from reaching other organs of our body (metastasis).
Lymph nodes are along the blood vessels and behind the pancreas.
Gallbladder cancer surgery
Radical cholecystectomy (extended cholecystectomy)
Surgery is the only treatment that has the potential for cure. Before surgery, we do staging workup to understand the stage of the disease.
The gallbladder is sometimes also removed for gallstone disease. In this surgery, only the gallbladder is removed. It is carefully separated from the liver. This surgery is called a cholecystectomy.
In surgery for gallbladder cancer, we remove the gallbladder with a chunk of the surrounding liver. Depending on the size or extent of cancer, the portion of the liver removed can be small or bigger. The draining lymph nodes which are along the adjacent blood vessels and pancreas are also removed. This procedure is called extended cholecystectomy or radical cholecystectomy.
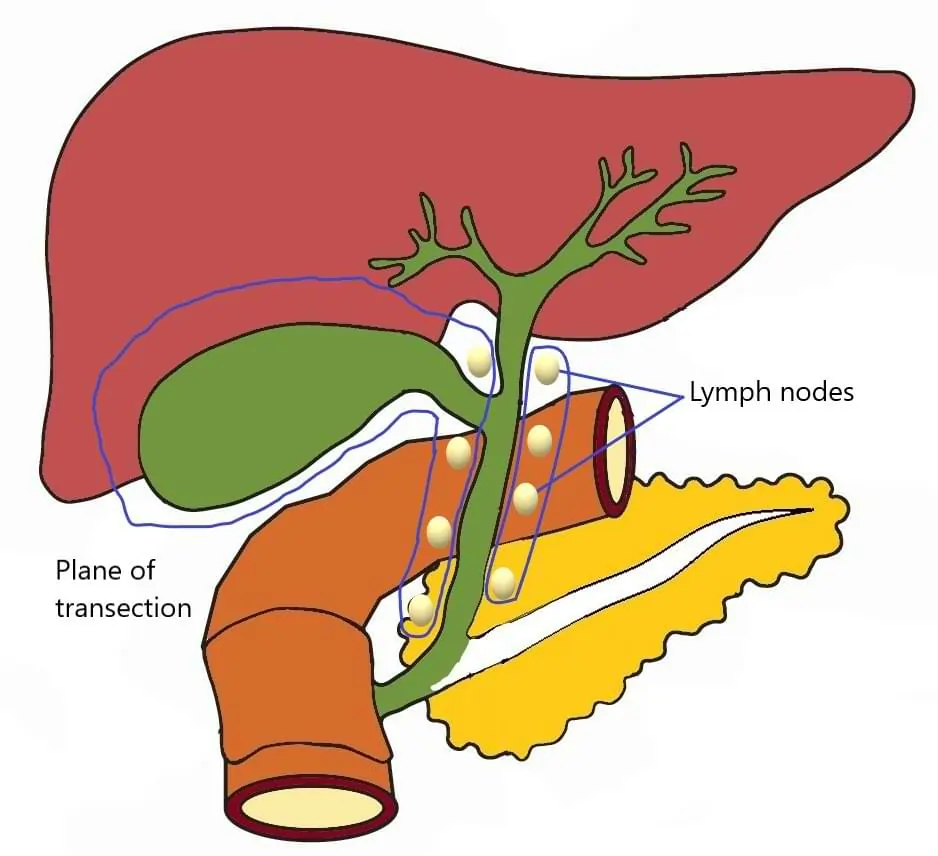
The parts encircled in blue line are removed.
Before proceeding with surgery, we always ensure that the disease has not spread to other parts of the abdomen. For this, a staging laparoscopy is done. It means examining the abdominal cavity and organs with a thin slender camera, inserted inside the abdomen through a small hole.
The gallbladder attaches to the bile duct and is situated close to the blood vessels of the liver and part of the intestine called the duodenum.
Some advanced gallbladder cancers involve the bile duct. In such cases, the bile duct is also cut out. We restore the flow of bile to the intestine by joining the small intestine to the remnant bile duct (Roux-en-Y hepaticojejunostomy).
Liver resection (hepatectomy)
If the tumour involves a large part of the liver or the blood vessel supplying part of the liver, the surgery will entail removal of that part of the liver, a procedure called liver resection or hepatectomy.

The parts encircled in blue line are removed.
Incidental gallbladder cancer
Many gallbladders are removed for gallstone disease. All such gallbladders are sent for biopsy, which sometimes finds cancer. This is called incidental gallbladder cancer.
The biopsy will also tell us about the T stage. T stage means how far cancer has spread into the layers of the gallbladder wall. We also do a CT or PET scan for staging.
If the T stage is T1b and beyond, then in such cases, the surgery is done. This is called completion extended cholecystectomy. In this, the liver around the gallbladder bed and adjacent lymph nodes are removed.
Sometimes, we also need to remove the bile duct and the laparoscopic port sites.
Laparoscopic or robotic gallbladder cancer surgery
Gallbladder cancer surgery is complex and requires experience. It is conventionally done through open surgery.
In open surgery, a single long incision is made over the abdomen to do the surgery.
The robotic or laparoscopic approach for gallbladder cancer uses minimally invasive techniques to do the same surgery with tiny incisions. This entails the insertion of special long, thin surgical tools through these small holes. It results in faster recovery and reduced pain compared to conventional open surgery. This requires expertise.
Robotic Surgery
Advanced Gallbladder cancer is an aggressive cancer with poor outcomes. Hence, Laparoscopic surgery in gallbladder cancer is usually restricted to early cancers only.
Anticipatory extended cholecystectomy
When we see a wall thickening of the gallbladder, which we suspect cancer but there is a possibility of it being noncancerous as well. In such cases, we remove The gallbladder with the wedge of the liver and send it to a frozen section (the pathologist will examine it for cancer). If cancer is present, lymph nodes are also cleared.
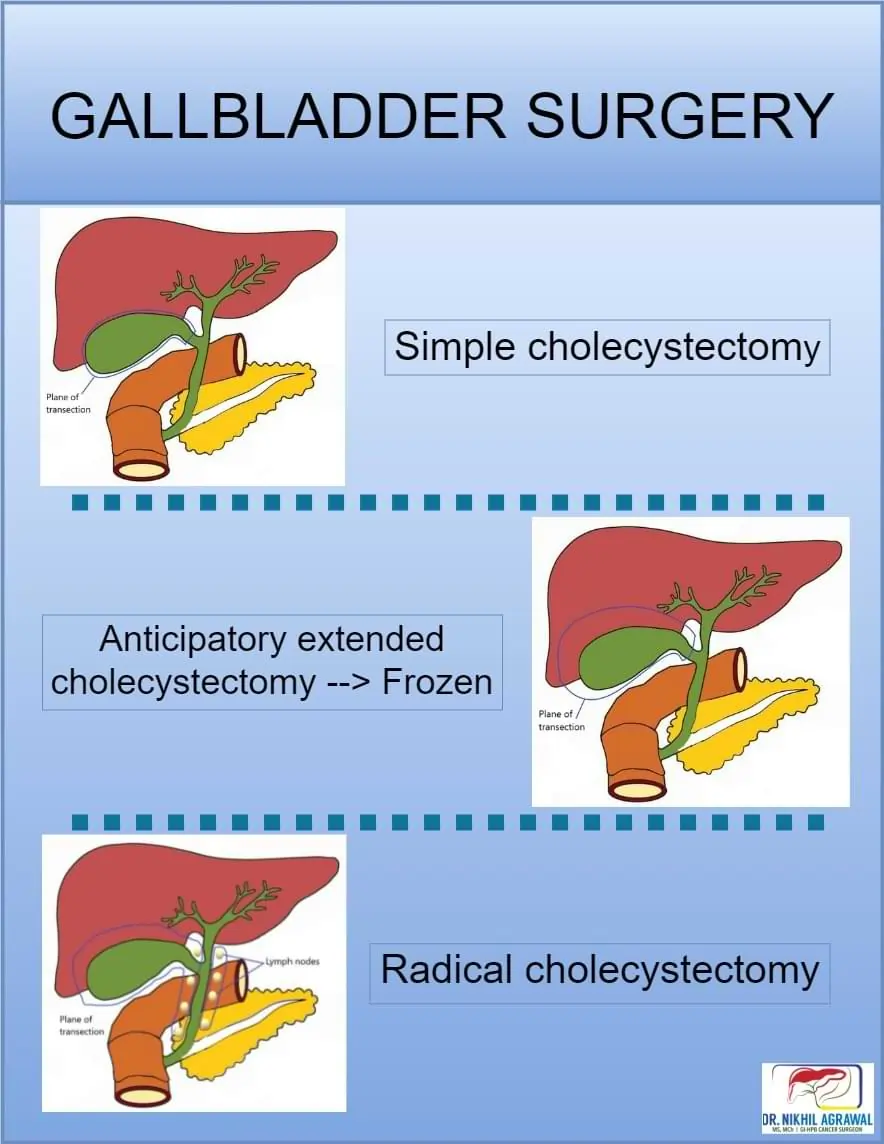
Types of gallbladder surgeries
Risks (complications) of gallbladder cancer surgery
All surgeries can be associated with complications and so is the case with gallbladder cancer surgery. Some common possible complications after gallbladder cancer surgery include:
- Bile leak: the bile ducts can leak.
- Infections - surgical site, pulmonary: Infections can occur after the surgery.
- Cardiac complication: Heart-related complications
- Bleeding: There can be bleeding during or after surgery
- Injury to adjacent organs: Many internal organs are very close to the gallbladder. They can be injured during surgery.
- Anaesthesia related complications: There can be complications related to the administration of anaesthesia and recovery.
- Postoperative obstruction: Post-surgery intestines can stop working, a condition known as postoperative ileus. They can get stuck or entangled, requiring surgery.
- Deep venous thrombosis: Clots can form in the veins of the leg due to immobility. These clots can travel to the lung also.
- Hernia: Hernia can form at the incision site.
Before surgery
The following steps will be taken to ensure the best outcome.
- Tests related to diagnosis, staging and surgical planning
- Tests related to fitness for surgery
- Optimising coexisting illness: Those with pre-existing illnesses such as diabetes, hypertension, cardiac disease etc. will be optimised to the best possible health.
- Admission
Can read more about preparing for surgery here.
After surgery
You will be closely monitored while you recover. It generally goes through the following steps.
- Intensive monitoring: Monitoring takes place in the ICU or recovery room
- Removal of tubes (Nasogastric, Foley and drain): Few tubes are placed during the surgery to facilitate the recovery. They are removed sequentially.
- Start and increase the diet: The oral intake is started with clear fluids and increased to a liquid diet and soft diet over a few days.
- Discharge: Once you are fully mobile and oral intake is adequate you will be discharged with instructions to follow at home. This usually happens 4-6 days after surgery.
- Follow-up: A follow-up visit is planned a week or 10 days after discharge. Clips or stitches over the incision are removed. The final biopsy report and further treatment plans are discussed.
Detect Early, Treat Right, Save Lives!

About Author
Dr. Nikhil Agrawal
MS, MCh
Dr. Nikhil Agrawal is a leading GI-HPB Surgical Oncologist with 20+ years of experience in complex cancers of the esophagus, stomach, colon, rectum, liver, pancreas, gallbladder, and bile ducts. He leads the GI-HPB Oncology Program at Apollo Hospitals, Delhi and Gurugram, with expertise in advanced robotic and laparoscopic cancer surgery.
His practice focuses on evidence-based, multidisciplinary care with an emphasis on individualized treatment and long-term outcomes.
He trained at BHU, SGPGI Lucknow, AIIMS New Delhi, and SNUBH, South Korea, and is a robotic surgery proctor who trains surgeons in advanced GI-HPB cancer surgery. He is also regularly invited as faculty at national and international scientific meetings.
This website helps patients and families understand GI and HPB diseases and cancers, treatment options, and what to expect during recovery and long-term care.