Laparoscopic Management of Suspected Gallbladder Cancer: Risk Stratified Approach in Thick-Walled Gallbladder and Polyps
Graphical summary
Laparoscopic Management of Suspected Gallbladder Cancer: Risk Stratified Approach in Thick-Walled Gallbladder and Polyps
Cite: Agrawal, Nikhil et al. "Laparoscopic Management of Suspected Gallbladder Cancer: Risk Stratified Approach in Thick-Walled Gallbladder and Polyps." Annals of surgical oncology, 31 Jul. 2025, doi:10.1245/s10434-025-17989-0.
Article (accepted version)
Ann Surg Oncol. 2025 Jul 31. doi:10.1245/s10434-025-17989-0.
Laparoscopic Management of Suspected Gallbladder Cancer: Risk Stratified Approach in Thick-Walled Gallbladder and Polyps
Agrawal N, Singh A, Jain M, Arora A, Chaturvedi HK, Pareek T
Correspondence: Dr. Nikhil Agrawal, GI-HPB Surgical Oncology, Max Super Speciality Hospital Saket, New Delhi
Email: drnkhl@gmail.com
Conflict of interest/ funding: None
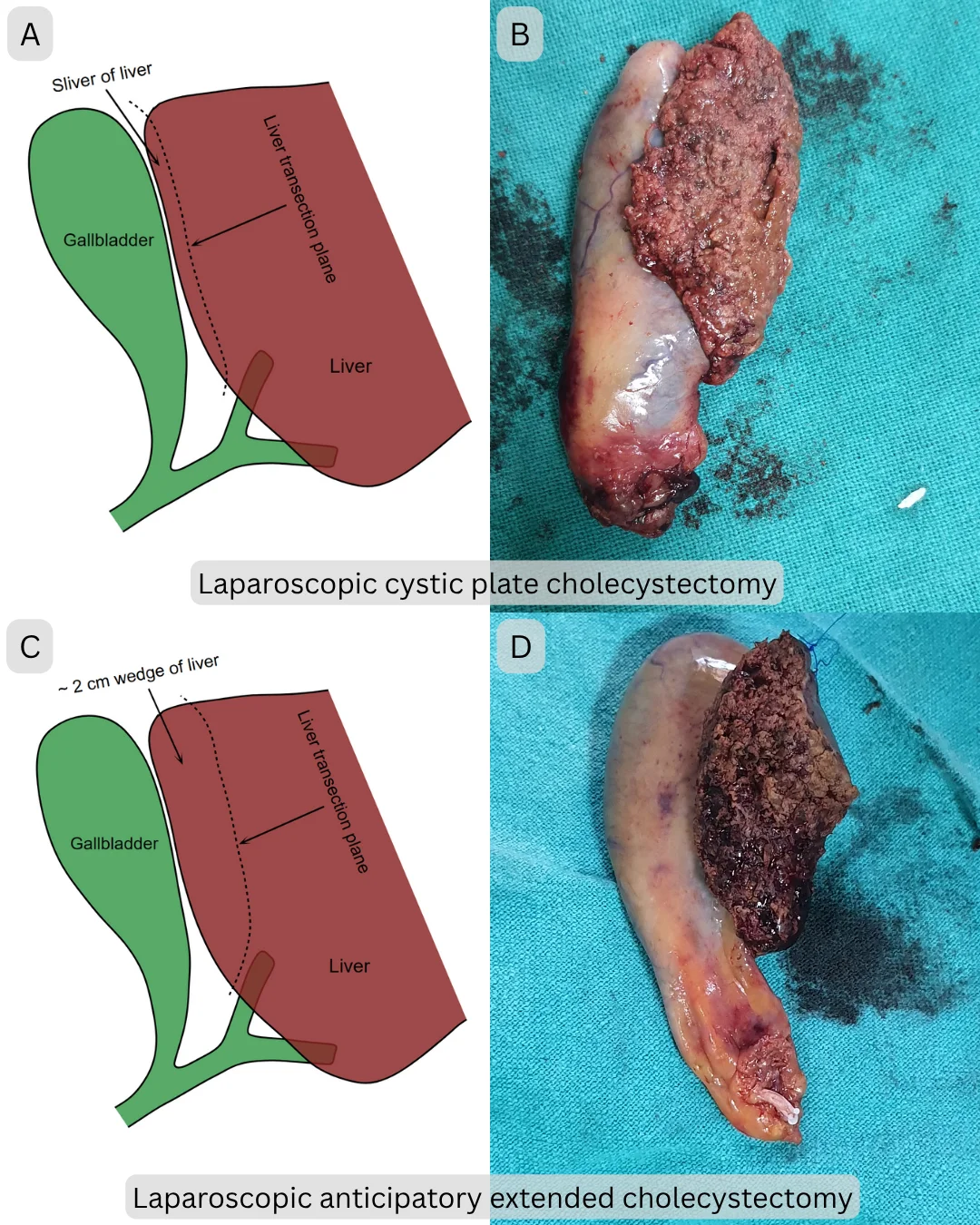
figure 2: A. and B. Graphical representation and operative photograph of laparoscopic cystic plate cholecystectomy. C. and D: Graphical representation and operative photograph of laparoscopic anticipatory extended cholecystectomy


Abstract
Introduction:
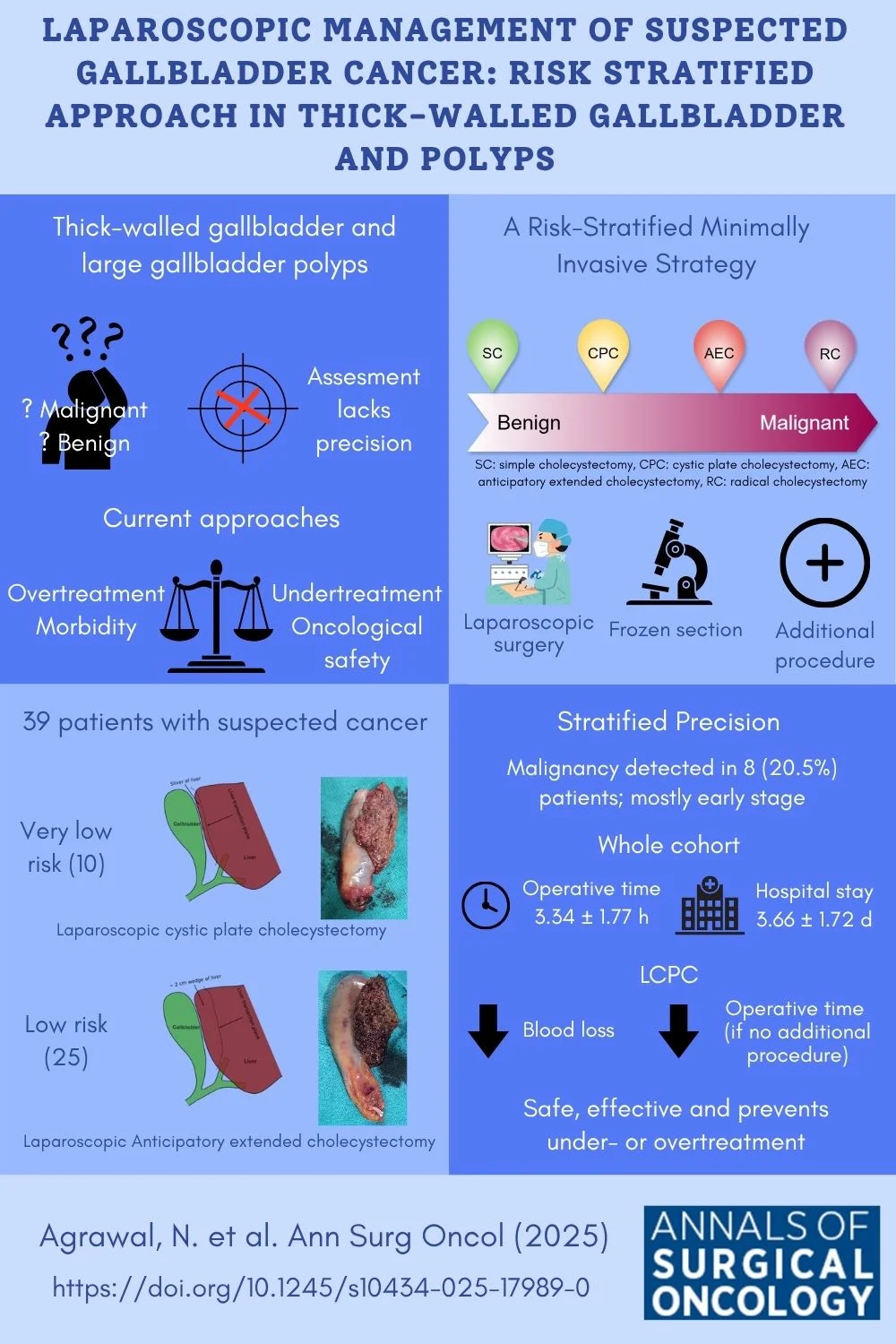
Thick-walled gallbladder (TWGB) and gallbladder polyps (GBP) can harbour cancer. Differentiating benign from malignant is challenging due to the limitations of diagnostic studies and unreliability of predictive models. Simple or radical cholecystectomy, pose risks of either inadequate oncological clearance or overtreatment. While anticipatory extended and cystic plate cholecystectomy with frozen section is useful but has limitations and laparoscopic approach with risk stratification is not well documented.
Methods:
In this retrospective study, 39 patients with TWGB or GBP suspected of malignancy were stratified into very low-risk and low-risk based on clinical, radiological, and intraoperative findings. Those with very low-risk underwent laparoscopic cystic plate cholecystectomy (LCPC), while those with low-risk underwent laparoscopic anticipatory extended cholecystectomy (LAEC). If frozen section showed malignancy, additional surgical procedures were carried out.
Results:
Of the 39 patients, 25 underwent LAEC, 10 LCPC and 4 simple cholecystectomies. Eight patients (20.5%) had cancer on frozen and underwent completion surgery. The mean operative time was 3.34 ± 1.77 hours, and the mean hospital stay was 3.66 ± 1.72 days. Clavien-Dindo = 3 morbidity occurred in four patients (10.2%).
Conclusion:
Managing TWGB or GBP with suspicion of cancer requires balancing oncological safety with overtreatment. A risk-stratified laparoscopic approach with frozen section is safe and effective.
Keywords: Gallbladder Neoplasms; Cholecystectomy, Laparoscopic; Risk Assessment; Gallbladder Diseases; Frozen Sections
Introduction
Thick-walled gallbladder (TWGB) and larger gallbladder polyps (GBP) can be associated with gallbladder cancer (GBC). Differentiating between benign and malignant cases can be challenging due to the limited accuracy of diagnostic studies including cross-sectional imaging and predictive models.
A simple cholecystectomy (SC) may compromise oncological outcomes by disrupting tissue planes in malignant cases. Conversely, performing radical cholecystectomy (RC) on all patients would cause overtreatment, unnecessarily exposing benign cases to increased morbidity and mortality.
As a balanced approach Kapoor et al.1 proposed anticipatory extended cholecystectomy (AEC), while Patkar et al.2 described cystic plate cholecystectomy (CPC) as an initial step, both incorporating intraoperative frozen section analysis. Additionally, patients with early gallbladder cancer benefit from the minimally invasive approach, reducing both morbidity and hospital stay as demonstrated by Navarro et al.3
AEC or CPC differ in the amount of liver parenchyma resected and has limitations. These relate to the problem of violating tissue planes and overtreatment if we use either of the procedure for all patients. Moreover, they have not routinely been described laparoscopically.
Therefore, we propose that by stratifying patients with a novel approach along a risk continuum and adopting a laparoscopic approach we can minimize operating time, morbidity and hospital stay. This is likely to improve outcomes. We can either do laparoscopic cystic plate cholecystectomy (LCPC) or laparoscopic anticipatory extended cholecystectomy (LAEC) depending on the risk of cancer. If an intraoperative frozen section confirms malignancy, completion surgery can be performed laparoscopically or via an open approach.
Patients and Methods
This retrospective study evaluated the efficacy of laparoscopic management using a risk-stratified approach in patients with TWGB or GBP with suspicion of cancer. Data were collected from the Department of GI-HPB Onco Surgery at Dharamshila Narayana Superspeciality Hospital, New Delhi (June 2018 to December 2019) and Max Super Speciality Hospital, Saket, New Delhi (November 2018 to April 2024) in India. The ethical guidelines for human studies were followed.
We categorized patients with TWGB and GBP along a spectrum of malignancy risk: likely benign, very low risk, low risk, and high risk (Fig. 1). Due to the lack of accurate objective criteria, malignancy risk was determined based on the treating surgeon's subjective assessment of clinical features, imaging characteristics, tumour markers, and intraoperative findings. The surgical team comprised of three experienced GI-HPB surgeons with each having over 10 years of expertise in managing such cases.
This study included 39 patients with very low to low risk of malignancy. Likely benign and high-risk patients were excluded.
Clinical characteristics, including demographics, comorbidities, and imaging findings (ultrasound, CT abdomen, MRI, or PET-CT), were collected. CA 19-9 values, operative findings, surgical procedures, frozen section results, postoperative outcomes, and final histopathology reports were also recorded. Independent two-sample t-tests were employed to assess the differences in means for these continuous variables.
Those with a very low risk of cancer and clear planes with the liver on imaging underwent LCPC, while those with a low risk underwent LAEC (Fig. 2).
The procedures were performed using standard laparoscopic techniques with four ports. A thorough staging laparoscopy was done to rule out metastasis. In LCPC, a small sliver of liver including cystic plate was removed with the gallbladder. In LAEC the gallbladder, along with an approximately 2 cm wedge of liver from segments 4b and 5, was removed (Fig. 2). Lymphadenectomy was not performed. The specimen was retrieved in a specimen retrieval bag or after the application of a wound protector and sent for frozen section analysis.
If the frozen section was positive for malignancy, patients who underwent LAEC proceeded to standard lymphadenectomy for gallbladder cancer, while those who had LCPC underwent completion radical cholecystectomy, including both liver wedge resection and lymphadenectomy. This was performed laparoscopically or via an open approach depending on the complexity of the case and preference of the surgeon.
Results
The mean age of the patients was 60.1 years (range: 33-87 years), with 21 males. In the LAEC group, six patients were found to have a malignancy in the frozen section and subsequently underwent lymphadenectomy. Frozen section analysis was performed in 9 out of 10 patients who underwent LCPC, and all were benign (Table 1). One patient sustained a bile duct injury, requiring an open Roux en-Y hepaticojejunostomy. Frozen section was not performed for one patient as the liver was found to have gross cirrhosis during surgery and we have not prepared and counselled her of the risks of surgery. The final histopathology revealed xanthogranulomatous cholecystitis (XGC).
Four patients underwent laparoscopic simple cholecystectomy (LSC). They had frozen Calot's and dense adhesions with adjacent organs and we suspected them to have XGC and hence resorted to LSC. Two cases were positive for malignancy and they underwent open completion radical cholecystectomy. Two cases were benign and had a cholecystoduodenal fistula and required duodenal repair (one open and one laparoscopic).
Apart from planned completion open surgery for malignancy, 2 out of 39 (5.12%) patients were converted to open surgery (1 - Roux-en-Y hepaticojejunostomy; 1- duodenal fistula repair).
Frozen section analysis revealed malignancy in eight patients. Among them, three underwent laparoscopic completion lymphadenectomy, three underwent open lymphadenectomy and two underwent open completion radical cholecystectomy. Additionally, two patients were detected to have adenocarcinoma in the final histopathology; one had T1a disease, and another had a 2 mm focus of adenocarcinoma. Both were advised observation, as their conditions did not warrant further surgical intervention. Most patients had node-negative T1 and T2 disease, except for one patient with T3N1 disease (Table 2).
The frozen section demonstrated an accuracy of 94.74% and a specificity of 100.0% in detecting malignancy. However, its sensitivity was slightly lower at 80.0%, with a negative predictive value of 93.33%. Though it missed two cases of invasive cancers, these were early cancers, and the performed procedure sufficed with no meaningful clinical impact.
The mean operative time for the entire cohort was 3.34 ± 1.77 hours. The difference in mean operative time between the LAEC and LCPC groups was not statistically significant (3.48 ± 1.45 hours vs. 2.25 ± 2.08 hours; p=0.0547). However, in patients who did not undergo an additional procedure, the operative time was significantly higher for LAEC compared to the LCPC group (2.84 ± 0.97 hours vs. 1.61 ± 0.54 hours; p=0.0016).
The mean blood loss for the entire cohort was 215.38 ± 208.42 ml. The mean blood loss in the LAEC group was higher compared to the LCPC group (208 ± 161.8 ml vs. 90 ± 45.9 ml; p=0.0023).
The mean hospital stay for the entire cohort was 3.67 ± 1.72 days. The mean hospital stay did not differ significantly between the LAEC and LCPC groups (3.4 ± 1.4 days vs. 3.6 ± 2.3 days; p=0.8). Patients who required an open procedure had a significantly longer hospital stay compared to those who underwent laparoscopic procedure only (4.88 ± 1.4 days vs. 3.35 ± 1.66 days; p=0.024).
Six patients had postoperative morbidity, of these 4 were Clavien-Dindo = 3 (10.2%)
Discussion
The differentiation between acute cholecystitis, chronic cholecystitis, XGC, and GBC based on imaging alone is difficult due to overlapping patterns. While cholecystitis typically exhibits diffuse, regular thickening, GBC often manifests as focal, irregular, and non-uniform thickening. Additionally, XGC and GBC can coexist, posing additional challenges in diagnosis and clinical management.
Gallbladder polyps are often detected incidentally during ultrasound examinations and their malignant potential remains debated. A systematic review by Mohamed Elmasry et al.4 analysed twelve studies and concluded that among 5482 GBPs, only 0.57% were malignant. Risk factors for malignancy included GBP size >6mm, single GBPs, symptoms, age >60, Indian ethnicity, gallstones, and cholecystitis. The reported incidence of malignancy is 8–10% for GBPs >10 mm and 1–3% for those measuring 6–9 mm.5
For cases where CT or MRI cannot clearly differentiate between benign and malignant thickening, additional studies such as FDG-PET and endoscopic ultrasound may be useful for further assessment.6 Despite advancements in radiological as well as endoscopic techniques, the ability to accurately characterize the malignant potential of GB wall thickening and polyp is still limited.
A thick-walled GB without suspicion of cancer can safely undergo SC. GBPs are usually observed and surgery is reserved for those at risk of malignancy. Patients with a high risk of GBC or proven malignancy should undergo RC. The dilemmas in decision-making arise in patients with very low to low risk of malignancy. One of the proposed strategies is to do a simple cholecystectomy followed by a frozen section.7 However, SC can potentially breach oncological planes, complicating subsequent surgeries, compromising oncological safety and leading to undertreatment if the final histopathology reveals GBC. It will also require an additional surgery.
In an analysis by Irrinki et al.8, Patients with missed carcinoma gall bladder who had undergone cholecystectomy had higher tumour stage, higher incidence of metastatic disease on evaluation, and a low rate of curative resections. Missed GBC had a poorer overall survival compared to incidental GBC (16.5 vs. 35.3 months; p=0.05).
Conversely, performing RC in all these cases would increase morbidity and operative time, leading to unnecessary overtreatment if the final histology is benign.
To address this concern Kapoor et al.1 proposed a novel surgical approach for such patients, termed AEC. AEC involves the removal of the gallbladder along with a wedge of liver tissue, with the specimen sent for frozen section histological examination. If malignancy is confirmed, additional lymphadenectomy is performed. AEC minimizes morbidity associated with lymphadenectomy and reduces the duration of surgery in cases where the disease turns out to be benign. However, it is still associated with significant morbidity and prolonged operative time and may not be appropriate for patients with a very low risk of cancer.
Another potential approach in these cases is to perform a cystic plate cholecystectomy (CPC) or full thickness cholecystectomy.2,9,10 A CPC avoids dissection in the perimuscular subserosal connective tissue plane, which is used in non-oncological cholecystectomy. This avoids violation of the tumour planes and gallbladder perforation. In CPC, a thin rim of liver tissue over the cystic plate is resected.
However, CPC can potentially breach tumour in those with liver infiltration and if the frozen section is positive for malignancy, a subsequent liver wedge resection is required, significantly increasing operative time. Hence, we used LCPC in only very low-risk cases without liver infiltration and only one patient in the LCPC was found to have malignancy (T1a), for which no additional surgical procedure was required.
AEC has traditionally been described as an open approach. However, a minimally invasive approach offers several advantages to the patient, including reduced postoperative pain, shorter hospital stays, and faster recovery. The laparoscopic approach in GBC is traditionally contraindicated due to fear of tumour dissemination and risk of port site metastasis. However, recent studies have negated this fear, particularly in early-stage diseases. Considering this, a laparoscopic approach in these patients can be considered safe3,11.
Our approach advocates the use of both LCPC and LAEC, with the choice of procedure stratified by the risk of malignancy. A risk stratified minimally invasive approach that incorporates both procedures has not been described previously. The Lower blood loss and shorter operative time (when no additional procedure is performed) in LCPC justifies its use in very low-risk cases, even though the hospital stay is similar. The Laparoscopic approach helps decrease morbidity and hospital stay. In our study, the mean hospital stay was 3.67 days, compared to a median hospital stay of 4 days in Kapoor's series. Notably, 23% of our patients were >70 years old and 48% had co morbidities. Patients who did not require an open procedure had a significantly shorter mean hospital stay (3.35 days) compared to those who underwent an open procedure (4.88 days; p=0.0076).
Intraoperative frozen section analysis is a reliable tool with high sensitivity and specificity for distinguishing benign from malignant and guiding appropriate surgical management. Chan et al. demonstrated that combining a surgeon's intraoperative assessment with frozen section analysis reduced unnecessary radical procedures and associated morbidity. All frozen sections were congruent with final histopathology but doubled the operating time.12 In our series, the frozen section missed two cases of malignancy (sensitivity: 80%). However, both were very early-stage cancers and the clinical impact was negligible.
In our series, the incidence of malignancy was 25.6%. In Kapoor et al.'s series, 2 out of 13 (15.4%) had malignancy, while in Patkar's series, 35.6% of gallbladders subjected to frozen section had invasive GBC.1,2 Except for one case, all our patients had node-negative disease with T1/T2 cancers.
However, the small sample size, retrospective design, and reliance on subjective assessment of malignancy limit the generalizability of our findings. An additional limination is the challenge posed by patients with frozen Calot's and dense adhesions to adjacent organs.
To conclude, we advocate a risk-stratified approach to patients with TWGB and GBP with suspected malignancy. These patients are categorized along a spectrum from benign to malignant (Fig. 1) based on clinical, radiological, and intraoperative assessments. Patients with very low and low risk of cancer should be treated with LAEC and LCPC (Fig. 2). We need larger prospective studies to develop objective criteria for risk stratification and validate their long-term efficacy.
References
- 1. Kapoor, V. K. et al. Anticipatory extended cholecystectomy: the 'Lucknow' approach for thick walled gall bladder with low suspicion of cancer. Chin. Clin. Oncol. 5, 8 (2016).
- 2. Patkar, S. et al. Utility and limitations of intraoperative frozen section diagnosis to determine optimal surgical strategy in suspected gallbladder malignancy. HPB 25, 330–338 (2023).
- 3. Navarro, J. G. et al. Oncologic safety of laparoscopic radical cholecystectomy in pT2 gallbladder cancer: A propensity score matching analysis compared to open approach. Medicine (Baltimore) 99, e20039 (2020).
- 4. Elmasry, M. et al. The risk of malignancy in ultrasound detected gallbladder polyps: A systematic review. Int. J. Surg. Lond. Engl. 33 Pt A, 28–35 (2016).
- 5. Aziz, H., Hewitt, D. B. & Pawlik, T. M. Critical Analysis of the Updated Guidelines for Management of Gallbladder Polyps. Ann. Surg. Oncol. 29, 3363–3365 (2022).
- 6. Ahmed, M. Clinical approach to patients with thick wall gallbladder. (2023).
- 7. Banh, S. et al. Single stage management of suspected gallbladder cancer guided by intraoperative frozen section analysis: a retrospective cohort study. Int. J. Surg. 110, 6314–6320 (2024).
- 8. Irrinki, S. et al. 'Missed Gall Bladder Cancer During Cholecystectomy - What Price Do We Pay?' An Experience of a Tertiary Care Center from India. Surg. Gastroenterol. Oncol. 28, 29 (2023).
- 9. Shirai, Y., Sakata, J., Wakai, T. & Hatakeyama, K. Full-thickness cholecystectomy with limited lymphadenectomy for gallbladder cancer. Hepatogastroenterology. 59, 1338–1340 (2012).
- 10. Kubota, K. et al. Laparoscopic cholecystectomy with full-thickness dissection for potentially cancerous lesions: comparison with standard technique. Hepatogastroenterology. 46, 3077–3082 (1999).
- 11. Ahmed, S. H. et al. Role of laparoscopic surgery in the management of gallbladder cancer: Systematic review & meta-analysis. Am. J. Surg. 225, 975–987 (2023).
- 12. Chan, B. K. Y. et al. Surgical management of suspected gallbladder cancer: The role of intraoperative frozen section for diagnostic confirmation. J. Surg. Oncol. 125, 399–404 (2022).
Table 1: Surgical procedures
| Procedure | n | Additional procedure | n |
|---|---|---|---|
| LAEC | 25 | Laparoscopic lymphadenectomy | 3 |
| Open lymphadenectomy | 3 | ||
| LCPC | 10 | Open RYHJ | 1 |
| LSC | 4 | Open completion radical cholecystectomy | 2 |
| Duodenal fistula closure* | 2 | ||
LAEC: Laparoscopic anticipatory extended cholecystectomy, LCPC: Laparoscopic cystic plate cholecystectomy, LSC: Laparoscopic simple cholecystectomy, RYHJ: Roux-en-Y hepaticojejunostomy
*One was done laparoscopically and another was converted to an open procedure.
Table 2: Frozen section and final histopathology
| Procedure | Frozen section | n | Final histopathology |
|---|---|---|---|
| LAEC | Malignant | 6 | Adenocarcinoma. T2aN0 (3) T1bN0 (1), T3N1 (1), missing (1) |
| Benign | 16 | Same | |
| Intracholecystic papillary neoplasm/ adenoma | 3 ± Same | ||
| LCPC | Benign | 8 | Same |
| Not sent (liver cirrhosis) | 1 | Benign | |
| Adenoma with high grade dysplasia | 1 ± Adenocarcinoma T1a | ||
| LSC | Malignant | 2 | Adenocarcinoma T2bN0 |
| Benign | 1 | Same | |
| Intracholecystic papillary neoplasm with low grade dysplasia | 1 ± 2 mm focus of adenocarcinoma T2Nx | ||
LAEC: Laparoscopic anticipatory extended cholecystectomy, LCPC: Laparoscopic cystic plate cholecystectomy, LSC: Laparoscopic simple cholecystectomy
This version of the article has been accepted for publication, after peer review but is not the Version of Record and does not reflect post-acceptance improvements, or any corrections. The Version of Record is available online at: http://dx.doi.org/10.1245/s10434-025-17989-0. Use of this Accepted Version is subject to the publisher's Accepted Manuscript terms of use https://www.springernature.com/gp/open-research/policies/accepted-manuscript-terms.

About Author
Dr. Nikhil Agrawal
MS, MCh
Dr. Nikhil Agrawal is a leading GI-HPB Surgical Oncologist with 20+ years of experience in complex cancers of the esophagus, stomach, colon, rectum, liver, pancreas, gallbladder, and bile ducts. He leads the GI-HPB Oncology Program at Apollo Hospitals, Delhi and Gurugram, with expertise in advanced robotic and laparoscopic cancer surgery.
His practice focuses on evidence-based, multidisciplinary care with an emphasis on individualized treatment and long-term outcomes.
He trained at BHU, SGPGI Lucknow, AIIMS New Delhi, and SNUBH, South Korea, and is a robotic surgery proctor who trains surgeons in advanced GI-HPB cancer surgery. He is also regularly invited as faculty at national and international scientific meetings.
This website helps patients and families understand GI and HPB diseases and cancers, treatment options, and what to expect during recovery and long-term care.