Robotic Completion Radical Cholecystectomy


Indication
Incidental gallbladder cancer
Patient Position and Port Placement
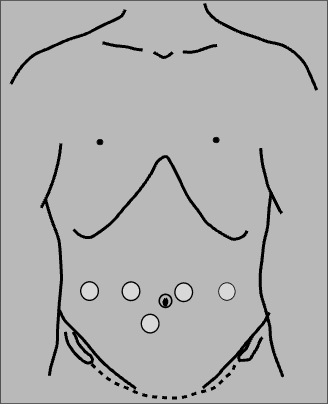
The patient is laid supine and in a Trendelenburg position with table slightly tilted towards the left.
Steps of Robotic Completion Radical Cholecystectomy
Robotic Incidental Gallbladder Cancer Resection
Adhesiolysis is done. We should follow the stomach and duodenum to avoid damaging the structures in the hepatoduodenal ligament.
Mesocolon of the hepatic flexure is detached from the duodenum and head of the pancreas.
The duodenum is delineated and Kocher's maneuver is performed.
The lesser sac is opened. The tissue over the right gastric artery is dissected. It will lead us to the proper hepatic artery.
Dissection is done around the proper and left hepatic artery.
The common hepatic artery is exposed and nodal tissue over it is dissected.
The left gastric vein is exposed and preserved.
The tissue covering the common bile duct is dissected, exposing the CBD.
The tissue between the proper hepatic artery and CBD is dissected exposing the portal vein.
The proper hepatic artery is encircled with a vessel loop.
The portal vein is located on the left side of the hepatoduodenal ligament.
All the nodal tissue on the left side of the hepatoduodenal ligament is dissected.
Dissection is extended to nodal tissue under the hepatic artery and to the left of the celiac axis. All the tissues are dissected out.
A window is created between the CBD and the portal vein. The tissue between CBD and portal vein is removed.
The right hepatic artery is dissected and demonstrated.
Dissection is performed to the right of the CBD, it is completely defined and the dissection is extended downwards to the right of the CBD.
The nodal tissue behind the CBD is detached from it and the CBD is encircled with a yellow vessel loop.
The dissection is continued behind the CBD and nodal tissue is separated.
The highest peripancreatic node and posterosuperior pancreaticoduodenal node are completely dissected and detached.
The cystic duct margin is revised and sent for a frozen section.
The line for liver transection is marked with monopolar scissor.
Stay sutures are taken on either side of the liver edge along the proposed transection line.
The liver capsule and superficial liver parenchyma is transected with monopolar scissor.
We can use the Maryland bipolar forceps to crush the liver parenchyma, similar to the technique used in Kelly clysis.
Smaller ducts or vessels can be divided using monopolar scissor.
The larger ducts or vessels are clipped and then divided.
The liver transection is brought closer to the hilum, and the liver parenchymal transection is then completed.
The specimen is placed in the retrieval bag and then taken out.
The cystic duct is sutured close with 5-0 PDS.
Hemostasis is checked, and a drain is placed.

About Author
Dr. Nikhil Agrawal
MS, MCh
Dr. Nikhil Agrawal is a leading GI-HPB Surgical Oncologist with 20+ years of experience in complex cancers of the esophagus, stomach, colon, rectum, liver, pancreas, gallbladder, and bile ducts. He leads the GI-HPB Oncology Program at Apollo Hospitals, Delhi and Gurugram, with expertise in advanced robotic and laparoscopic cancer surgery.
His practice focuses on evidence-based, multidisciplinary care with an emphasis on individualized treatment and long-term outcomes.
He trained at BHU, SGPGI Lucknow, AIIMS New Delhi, and SNUBH, South Korea, and is a robotic surgery proctor who trains surgeons in advanced GI-HPB cancer surgery. He is also regularly invited as faculty at national and international scientific meetings.
This website helps patients and families understand GI and HPB diseases and cancers, treatment options, and what to expect during recovery and long-term care.