Stage 4 colon and rectal cancer that has spread to the liver



Patients of colorectal cancer with liver metastasis do not survive long without treatment. With modern chemotherapy, they survive for 1-3 years. Patients with limited metastases who undergo surgery or other curative treatment survive much longer.
Colorectal cancer metastases
Colorectal cancer means cancer originating in the colon and rectum (large intestine). Colorectal cancer is the third most common cancer worldwide. It is among the top ten cancers in India and its incidence is increasing.
Cancers tend to spread. When cancer spreads from its organ of origin (called primary) to a distant part of the body, it is called metastases (secondary). It can be present during the initial workup when the cancer is first detected or can reappear later (recurrence) after the treatment of primary.
Colon and rectal cancer tend to metastasize to liver, lung, peritoneum, bones and distant lymph nodes.
Liver metastases
Liver metastases mean that cancer has spread to the liver. Colorectal cancer has the propensity to go to the liver. 35-55% of patients with colorectal cancer will develop liver metastases. One-third of these patients will have metastases confined only to the liver.
Liver metastases can be
As per the current cancer staging system (American Joint Committee on Cancer; AJCC), cancers with metastasis are classified as stage IV.
There is hope
Most stage IV gastrointestinal cancers do not have a long-term cure with currently available treatment modalities. However, many patients with limited colorectal cancer liver metastases and extrahepatic disease can have long-term survival and even cure with appropriate treatment. Surgical removal (resection) of colorectal cancer liver metastasis results in increased survival. Currently, the overall 5-year survival rate of operated colorectal cancer liver metastases is approximately 50-60%.
Each patient of colorectal liver metastasis is unique in its own sense depending on the location and stage of the primary tumour and the number, location, distribution, and volume of liver metastasis. Hence an individualised approach must be developed for each case.
Workup and staging
Once a colorectal liver metastasis is detected the workup is then focused on finding out the number and distribution of metastatic spots in the liver and their relationship with major blood vessels of the liver.
In synchronous tumours, the stage and location of the primary tumour in the colon or rectum and symptoms because of the primary are also important considerations in the decision-making process.
We also need to check whether there are any other spots in the body (extrahepatic disease).
The amount of liver going to remain after the resection is also calculated. This is called Future Liver Remnant (FLR). Though the liver can regenerate after surgery, adequate liver should remain for a successful outcome.
The following tests help us in complete evaluation:
CEA
Most colorectal cancers produce a substance called CEA (carcinoembryonic antigen). A blood test checks its level in the blood. It is a useful test for monitoring.
Computed tomography (CT) scan
In this, the patient is placed in a scanner and beams of X-rays image the inside of the abdomen from all sides. These images are then computer-processed giving an accurate representation. Contrast injected into the blood enhances these images.
Magnetic resonance imaging
Instead of x-rays, it uses radio waves and strong magnetic fields. MRI is highly accurate and our primary modality to understand the distribution of liver lesions. It is good in the characterization of subtle, less than one cm and indeterminate lesions. MRI also performs well in fatty liver, disappearing metastasis after chemotherapy and in assessment post-chemotherapy.
Positron emission tomography (PET) scan
Cancer cells take up a larger amount of glucose. Here, injected radioactive glucose (18F-fluorodeoxyglucose; FDG) binds to the tumour, and then the patient is scanned. The images are computer-processed and combined with CT images, giving us a CT image with bright tumours. It is mainly used to look for extrahepatic disease.
Intraoperative ultrasound
Ultrasound uses sound waves to produce images of structures. During surgery for colorectal liver metastasis, a specially designed ultrasound is used to assess the lesions. It provides high-resolution images as the transducer is in direct contact with the liver. It helps us identify small lesions not visible on MRI or CT and guides us to resect the lesion safely with adequate margins.
Besides, we also assess the fitness of the patient and his/her ability to withstand the treatment.
Treatment of colorectal cancer liver metastases
Not all patients with CRLM can be treated with curative intent. Approximately one-third of all patients with CRLM have a disease which can be removed. This sometimes requires multiple steps and a combination of multiple treatment modalities.
Surgery for stage 4 colon and rectal cancer spread to liver
Metastatectomy or Hepatectomy (liver resection)
We surgically remove the liver metastasis. In metastatectomy, we resect the liver lesion with a healthy margin. Hepatectomy is the removal of part of the liver containing cancer with healthy margins. It is done when the remaining liver after surgery is of adequate size and functioning well. The remaining liver grows over a few weeks.
For patients to undergo surgery we should be able to resect or ablate all the lesions safely (with adequate liver remaining after surgery).
Ablation
Ablation uses extreme heat, cold or chemicals to kill the tumour cells. This is best for small tumours which are less than 2 cm. Radiofrequency ablation (RFA) uses high-frequency radio waves to generate heat and kill the tumour. A probe is inserted into the tumour guided by ultrasound or CT scan. Microwave ablation uses microwaves to generate heat and kill the tumour. Cryoablation or cryotherapy kills the tumour by freezing it with a metal probe. Percutaneous ethanol injection (PEI) can also be given into the tumour killing the cells.
Stereotactic Body Radiation Therapy (SBRT)
The procedure uses many precisely focused radiation beams to treat tumours.
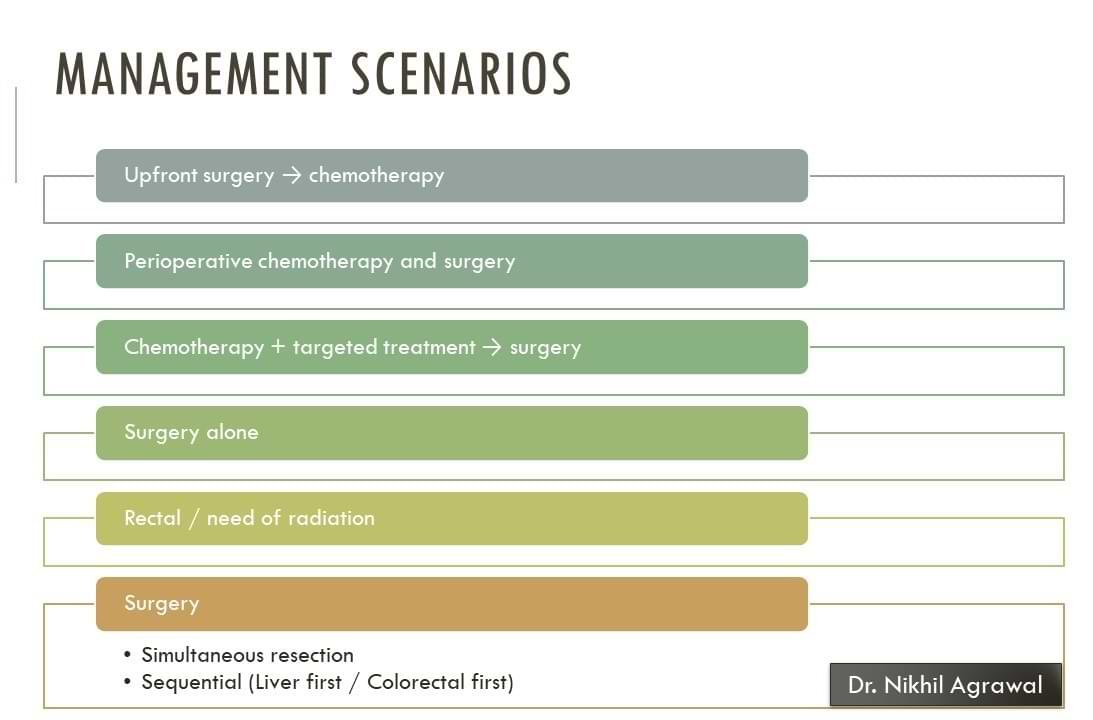
Treatment planning
Based on the distribution, number, volume, and location of these spots we determine the best strategy to treat them. There are many variations to this strategy. These variations in strategy depend on how advanced the disease is. Whether we are dealing with a synchronous or metachronous disease. How advanced the tumour is in the colon or rectum. Whether the colorectal primary is bleeding or causing obstruction or any other symptoms. If there are any metastatic spots outside the liver. If the primary tumour is in the rectum, we also need to employ radiation in the treatment plan.
In case of synchronous disease, we can operate both colon/rectal cancer and liver metastasis together or we can do both the surgery in stages. The choice depends on the magnitude of the surgery and the fitness of the patient.
Various other strategies are used to safely address all the lesions. Surgery can be combined with ablative procedures or SBRT to address all the lesions. Surgery can also be done in multiple stages to safely remove all the lesions. Modalities to increase the liver volume which is going to remain after surgery such as portal vein embolization also can be used. A newer technique to resect large amounts of the liver called ALPPS is also being introduced.
Perioperative, neo-adjuvant and adjuvant chemotherapy
Besides surgery, almost all these patients are administered chemotherapy. Sometimes a few cycles of chemotherapy are given before surgery and rest after surgery. Else, the chemotherapy is administered after surgery. This depends on the distribution, number, volume, and location of these spots in the liver.
Chemotherapy may help by reducing the size of lesions and potentially killing cells that are not seen. Progression of tumour on chemotherapy and increased risk of surgery following chemotherapy is a concern.
Targeted and immunotherapy
Targeted therapies are antibodies or drugs that inhibit specific proteins that are required for cancer cell growth. They attack cancer cells without harming normal cells. Targeted therapy is added to chemotherapy when the liver metastases are deemed unresectable and the aim is to shrink it and make it resectable.
There is an emerging role of immunotherapy in a subset of patients. These are patients who have deficient DNA mismatch repair (dMMR) genes or microsatellite instability-high (MSI-H).
Extrahepatic disease
Besides liver metastasis if the patient has a few cancer spots elsewhere in the body, we can still treat it with curative intent provided the disease outside the liver can also be addressed. Lung and ovarian metastases, locoregional recurrences of the primary tumour, portal lymph node, and limited peritoneal disease are amenable to curative treatment.
Prognosis (survival rate) of colorectal cancer liver metastases
Life expectancy for stage 4 colon cancer spread to liver
It is often measured as 5-year survival. It is the percentage of people with the same type and stage of cancer who are alive 5 years after diagnosis. These estimates are generated from many patients. Overall 5-year survival for stage 4 colorectal cancer is 15.7% (National cancer institute data). For patients in whom curative treatment, such as surgery is done, the 5-year survival approaches 40-60%.
With appropriate treatment, many of these patients with colorectal cancer liver metastasis will have a meaningful life span.
Early detection and appropriate treatment can save lives.
Stay Alert! Stay Healthy!
Wish you a speedy recovery!

About Author
Dr. Nikhil Agrawal
MS, MCh
Dr. Nikhil Agrawal is a leading GI-HPB Surgical Oncologist with 20+ years of experience in complex cancers of the esophagus, stomach, colon, rectum, liver, pancreas, gallbladder, and bile ducts. He leads the GI-HPB Oncology Program at Apollo Hospitals, Delhi and Gurugram, with expertise in advanced robotic and laparoscopic cancer surgery.
His practice focuses on evidence-based, multidisciplinary care with an emphasis on individualized treatment and long-term outcomes.
He trained at BHU, SGPGI Lucknow, AIIMS New Delhi, and SNUBH, South Korea, and is a robotic surgery proctor who trains surgeons in advanced GI-HPB cancer surgery. He is also regularly invited as faculty at national and international scientific meetings.
This website helps patients and families understand GI and HPB diseases and cancers, treatment options, and what to expect during recovery and long-term care.